Even two years after the last wave of the COVID pandemic went around the world, everyone still seems to be numb from the last experience. Click the image to expand it.

social, health, political imagery through the lens of G J Huba PhD © 2012-2021
Even two years after the last wave of the COVID pandemic went around the world, everyone still seems to be numb from the last experience. Click the image to expand it.
When Donald Trump ran for and won the US Presidency we all knew what we were getting. It was a clown show run by a guy who controlled the nuclear weapons, was grossly bigoted, kissed and discussed private lady parts, among many other crude and dangerous behaviors. He committed high crimes and misdemeanors against the country he promised to protect and make safe. Half of the country thought he was a great leader and the other half thought he was stealing money and goods from the country and ruining the reputation of the United States.
What the USA got was a Clown President who said he loved three dictators (from Russia, China, and North Korea), who tried to start several wars, said he loved many terrorist groups, refused to admit that the US was in a severe state of chaos during a pandemic that killed more a million Americans. He devoted much of his time and energy in trying to establish a lasting dictatorship in the USA.
What the USA got during the four-year term Trump. from 2017 to 2021 was a CLOWN-GAMESHOW-HOST.
Presenting Donald Trump, the President with no clothes and a yellow mop wig.
Just so you never forget, the following is the game board from the crazy years he oversaw.


December 22, 2022

It seems very obvious to me that the 2020 (now 2021) Olympics starting on July 23, 2021 should be a “no starter.”
Covid infection and death rates are again surging as Variant D spreads globally
Holding the Olympics could cost millions of lives. Worth it to you? Not to me.
Click the image to expand it.

Some other considerations.

Get vaccinated. Your risk of getting Covid-19 is going way up if you are unvaccinated. If you do not have access to vaccine, wear a mask, stay six feet away from others, stay out of crowds, and wash your hands.
Variant Delta (D or the Indian variant also well-established in the UK) is the most severe of all variants to date, and is becoming the dominant version of Covid-19 in many countries. Many public health professionals predict that within a few months Variant Delta will the dominant strain globally and in the USA, much as it is currently dominant in India and the UK..
If you want to see the most current information about Covid-19, Variant Delta, search with Google or an alternative search engine. As I write this on June 19, 2021, there is a huge amount of news stories available. CNN has had good coverage on Variant Delta.
Current information is that Variant Delta is the most problematic and deadly Covid-19 variant yet.


by George J Huba PhD (Psychology)
This weekend the American Psychological Association is meeting in San Francisco. While certainly not exclusively so, the meeting tends to be dedicated to the presentation of fairly trivial and limited scope, poorly designed research studies.
Psychology should be embarrassed that the focus of the meeting is not developing new and better ways of addressing psychological problems. For instance, I have dementia. So do many millions of people worldwide. At this psychological meeting, there is little focus on actually improving the lives of persons with dementia. The same is true for many other psychological disorders.
How has psychology failed persons with dementia? The following mind map presents my assessment of the situation.
Why does psychology fail persons with dementia? I believe it is because the field wants to pretend it is a science of the rigor of biology and physics, rather than focusing on becoming an evidence-based way of developing better ways of patient assessment, screening, treatment, and communication. What a waste. And remember that I am a person with degenerative cognitive and behavioral disease and I get it. Shame on psychology.
Click the image to expand it.

by George J Huba PhD (Psychology)
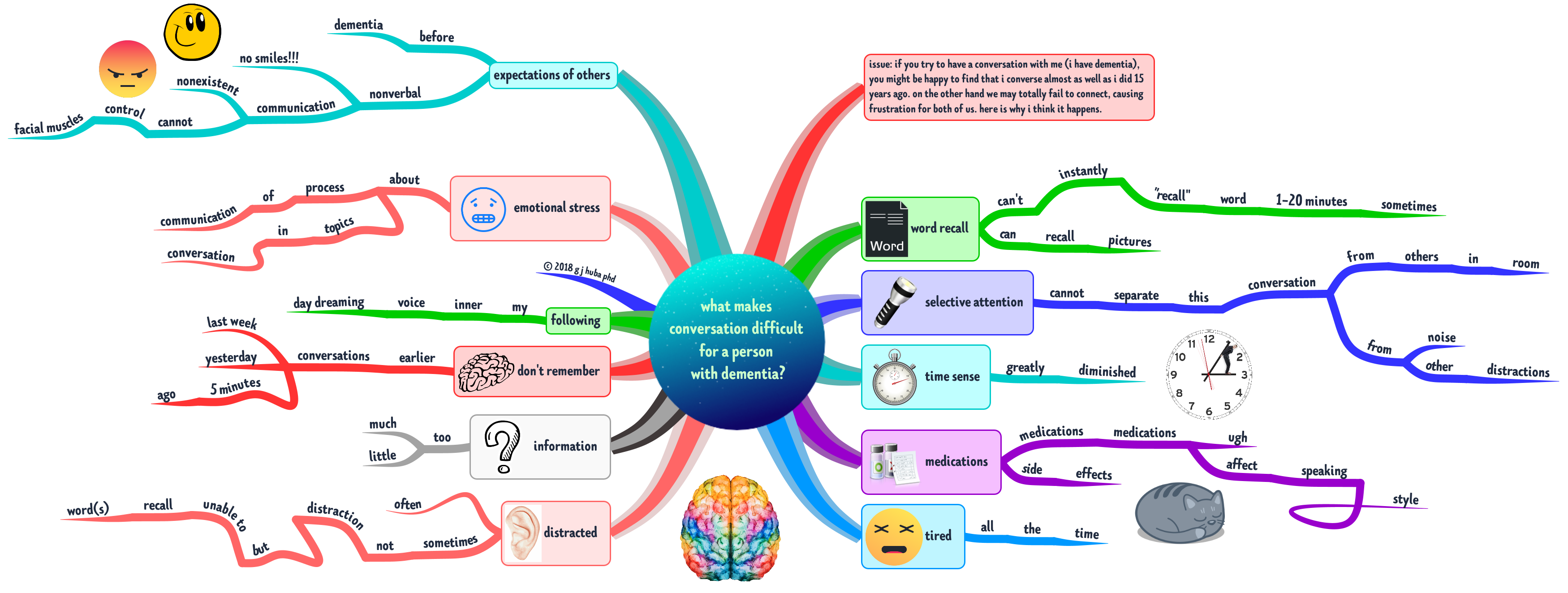
Dementia is a time that gets extremely complicated for a person with dementia and their spouse, family, friends, new social acquaintances, healthcare providers, and caregivers.
Probably the biggest issue is that those who interact with the person with dementia expect the PWD to communicate in a way that is diminished but still like the way a typical person without dementia communicates just now at a lower level.
It is difficult to communicate with a person with dementia because their own experience of communications is now shaped by the brain changes and other symptoms of dementia. What about your Mom who no longer smiles when you say something she has always liked or when you bring her the pistachio ice cream she has always loved? Ever consider the possibility that she thinks she is smiling but has no control over nonverbal communication such as her smile. Brain damage of various types can cause the loss of nonverbal communication abilities or control of facial muscles.
Why does your friend always get overwhelmed and say something stupid when there are lots of other people around? Perhaps they can’t focus on what you are saying because there is so much noise and motion from distracting sources?
Ever wonder why your friend with dementia comes back with an answer to a question five minutes after you asked the question? Brain changes and damage during dementia may make it hard to retrieve information or think and a loss of a sense of time may mean your friend keeps working on answering the question long after the conversation has moved on.
In dementia, a daydream may be as vivid as something in the real world, and just as distracting. In dementia, you can’t deal with too much information because it distracts you and can’t “fill in the blank spaces” if you receive too little because your “executive functioning” has been destroyed. You tend to get anxious during a conversation not only from unpleasant topics but also from worrying so much about missing a word or forgetting a name or misinterpreting a suggestion as hostile when it was just a normal joke.
The physical and psychological consequences of dementia combine to make it seem that a person with dementia is speaking a different language. They are.
And yes, those 20 or more pills the person with dementia may take daily can affect the ability to speak clearly, pay attention, be sleepy, look like they are bored when they are not, or become even more anxious.
Additional thoughts are arranged on the mind map below.
Click on the image to expand it.
Always try to remember that the person with dementia is often not disinterested or misunderstanding you or too tired to think or extremely distracted in what you think is a peaceful environment.
And if you are a person with dementia, remember that your friend is not trying to mislead you or express hostility and disapproval. They are not trying to trick you or harm you or pick a fight. You might not remember a conversation your caregiver says you had 10 minutes ago, so get over it and trust the other person. Nobody is criticizing you as a person because you can no longer tie your shoelaces or your necktie.
All parties in a conversation with a person who has dementia need to realize that the “rules” for the social encounter have changed because of the disease. Both persons with dementia and their families and friends and caregivers need to realize that is just as hard for all parties to figure out this new “language of dementia.” But it can be done and when mastered can liberate everyone to some degree.
Learn to laugh and smile and enjoy the company of each other again. The positive emotions are still there but they may have to be expressed in different ways. Learn how to express oneself when one or more parties has dementia. It’s worth the time. For everyone.
#mindmap #mindmapping #dementia #Alzheimers @DrHubaEvaluator
The #1 thing that I have learned over almost a decade of living with dementia is that thinking in pictures (images, diagrams, doodles, etc.) is much more effective than using words alone. Hedge your bet. Use pictures that associate with words rather than just words. After all, in many types of dementia, you lose your words at the end while the pictures may escape loss.
Try it. You will probably like it. Creating visualizations of important events, ideas, feelings, and other information can be FUN.
I’ve been using visual thinking methods for the past 10 years. They work (for me).

Last week (June 14, 2017) I received an email from a close friend with a link to an article generated by the North Carolina station of the National Public Radio a month ago. Along with noting that the research process was not what it once was — specifically that I had received a description of a study carried out in India from a psychologist in Israel with a summary of a radio broadcast generated about five miles from my home.
The changes in how we think, process and access information, and communicate change dramatically annually (as well as monthly, weekly, daily even). But is everyone changing how they fit to match our modern world and its information use possibilities?
People of many different income, education, social, and other strata within Indian society took EEGs to study their alpha brain patterns. There were many differences between the way that their brains seemed to work as measured by EEG indicators that could potentially be explained by differences in exposure to different levels and kinds of technologies.
A summary of the work appears here and was written by the University of California, Berkeley, philosopher Alva Noe. Noe discusses how brain wave patterns may have changed as individuals are exposed to the dramatic new information access and processing annually. The original scientific research by and appears here. Noe notes that one of the “problems” in our current conceptions of neurocognitive science is that virtually all of the experimental results have been derived from “WEIRD” brains, that is individuals educated in current technologies within western, industrialized, rich democracies. The Indian results suggest that there are different patterns of “NORMAL” brain waves among individual from other backgrounds.
I find Noe’s ideas to be quite compelling.
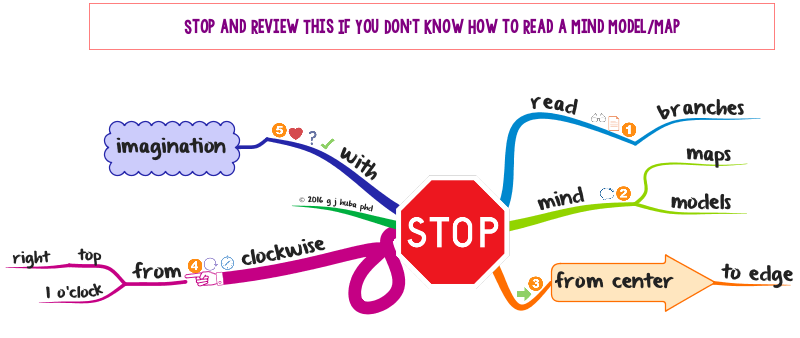
Click to open the mind model (aka mind map).
Many criticize the Trump White House as disorganized. Trump Land is already using the following color coding scheme they seem to have developed; they should make it public so that the public can see how they treat their friends and not-friends.
Click the image to expand.

There are many kinds of dementia, but in many types, one huge change is that you lose partially or fully the ability control your facial expression, body posture, and other physical movements that indicate to another person how you feel, how attentive you are, sudden joy, fear, and especially empathy.
Since my diagnosis of FTD (and several years before that), I have heard statements like these from strangers, friends, and family members. Many people think I am angry, disinterested, or not listening to them.
“You never smile.”
“We’re waiting for you not to frown so we can take the selfie.”
“You don’t care what I think, all you do is look at me with a smirk on your face.”
Well, most of the time I am happy and/or neutral although I am sometimes depressed to varying degrees. I am usually interested in what most people are saying. Sometimes I have to break into conversations multiple times to say that I am confused. That confusion is, for me, more likely to indicate that I cannot decode your words because I am losing language skills, not because I was not paying attention to you. I slouch a lot, I often walk looking directly down because I easily trip over over cracks in the pavement and that sometimes leads to falls (I am currently typing using my left thumb on the spacebar because I broke my right thumb in a fall a month ago).
You cannot judge how I am feeling physically or mentally by looking at me unless you are part of my core family and see me very often and sometimes not even then.
That sucks.
Much of how we feel about people is based on their nonverbal gestures and facial expressions. Somebody like me who can barely smile gives people the impression they don’t like what is being said or are annoyed or distracted.
Most people infer negative things from my posture and face and staring that are simply not true.
This is probably a huge factor in how miscommunications often occur among persons with dementia and those they interact with. Even people who interact with me regularly and know my medical problems often misinterpret me.
The following mind model shows some issues in communicating with persons with dementia and possibly misinterpreting what they are thinking and feeling because they look at you with unintended disinterest, never smile, and look distracted. People have often misinterpreted my attempt to smile as smirking.
And if you are a person with dementia, look at yourself in the mirror or in recent photographs and see if you can make some improvements in facial expressions and posture. And if not, when you talking to people, especially friends and family, remind them that you not in complete control of your facial expressions and that sometimes when you think you are smiling or even grinning, the other person just sees a blank face. You can also make a joke out of the situation.
Click on the mind model image below to expand it.

Have a good day.
A phrase you have heard thousands of times (especially if you have lived in California as I did for 30 years). If you have dementia you may groan or the statement may make you angry or you might make a pointed comment back.
Chill, Dudes and Dudettes.
OK, I get it (well actually have gotten it for a number of years since diagnosis). There may not be a 100% good day for you anymore if you have dementia. But how about a perfect (or even good) 20 minutes having coffee with a friend or an hour solving a puzzle with a grandchild or 100 minutes watching Guardians of the Galaxy 2 complete with a refillable tub of popcorn. Yup, these periods of a good day may be followed by a period of frustration or not being able to remember something or difficulty doing a task of daily living.
Use the Force, Luke.
Good moments can be great moments if you let them be. They may last only for few minutes or an afternoon, but given that your brain is “sick” they are a huge gift and blessing. Focus on what is happening to you now, try to not let the bad upset you unduly, and try to enjoy every moment for every second possible.
You may master the Force. You may feel better. Is there a better use of your time?
Focus on what is, not what was.
Click the image of the mind model (mind map) to expand it.

ObamaCare revised/enhanced?
Trump/RyanCare another draft not submitted to Congress?
Within the extant and mythical healthcare plans, additional dementia care services need to be included. Most are cost-neutral or may actually save money while providing better patient outcomes.
Case Management makes existing healthcare services (doctor visits, medications, emergency care) work better. At a very small cost that should actually SAVE money, case management can provide better total patient care, cut unnecessary emergency room visits, and achieve better medication outcomes. What isn’t there to like?
Dementia Caregivers are most often UNPAID, female family members forced to juggle their own jobs/finances, families, and general lives to care for a loved one. Support is required for Dementia Caregivers in the forms of training, support, advice, and FINANCIAL COMPENSATION for their services. They do the work, they should get paid for their time. An upgraded system of paid family caregivers should make DementiaCare more effective and reduce other costs in the healthcare system to such a degree that it will be cost-neutral. An unnecessary hospital stay or emergency room visit can cost as much as $10,000 — $20,000. A family caregiver could be paid for 500 hours at $20 per hour for $10,000. Train family caregivers, pay them, and you have a cost neutral system. What isn’t there to like?
Mental Health issues often lead to huge patient distress, anxiety, and medical management problems. They can frustrate caregivers and lead to nonadherence to medication recommendations. Therapy and counseling can help patients and caregivers as well as cutting overall medical costs. What isn’t there to like?
Group Adult Daycare can provide needed respite for family caregivers as well as important social and recreational experiences for patients, thus enhancing their lives and to some degree ability to function independently. What isn’t there to like?
The following mind model provides some details. Click the image to expand it.

I get in trouble when I make mind maps about Donald Trump. This is a mind map about processing repetitive TV cable news (on CNN and MSNBC and FOX) about the most televised story — Donald Tackles the USA and the World — at this point in late April 2017.
Mr Trump is just completing the first 100 days of his Presidency having accomplished less — according to the fact checkers from numerous news organizations — than any President since the index has been tracked from the beginning of Franklin Roosevelt’s Presidency in the 1930s. Mr Trump believes he has accomplished more than any president ever studied in his first 100 days.
I am a lover of news stories where the President gets bashed on TV. In the 1970s I watched (and read about) all the hearings focusing on Richard Nixon and Watergate. In the 1980s I watched huge amounts of TV about Reagan and Iran-Contragate. In the 1990s, I watched the hearings about Bill Clinton and the blue dress and impeachment and not inhaling. Nothing of a comparable nature occurred during either Bush presidency or that of Barack Obama. I almost didn’t know what to do with my spare time.
Now, I am watching numerous hours of TV/video on the major USA news channels (including CNN, MSNBC, Fox, CBS News online, New York Times, Washington Post, and of course the best news outlet for all news worldwide, BBC). And even ESPN has had a big Trump story about star players declining invitations to the White House to meet POTUS.
My dementia has been progressing at an ever increasing speed in a downward spiral during the past months. I remember (recall) less from current events and “work” and daily tasks. When I can retrieve information I do so very S—L—O—W—L—Y. Judgments are tougher, understanding sequences are harder, and writing down what I think is very slow as the length of my current journal entries (and al of the wurds nat spelled wrongly or too bigly) is increasing grately. Handwriting does not come with A spel chkr.
The current trend in cable TV news on MSNBC and CNN and others is to have one-hour shows where a moderator/commentator discusses all of the “important” news of the day with 2-5 different “self-styled” experts ranting from all political persuasions.
7 hours of liberal rantings about Trump is available on MSNBC and to a lesser degree on CNN; Fox News has 7 hours of conservative rantings about how terrible it is that the liberals are ranting about Trump.
I have repeatedly argued that inexpensive (or even free) visual thinking/mind modeling methods can help a person with dementia “rewrite the operating system” on that storage device we call the brain and think better, albeit in a different way.
As I was making the following mind model (AKA mind map) about Trump’s first 100 days yesterday, I was struck by how rapidly I could create this fairly complex model. I think it shows that the intrinsic interests and REPEATED exposures to structured, summary information can be well captured using visual thinking methods by a person who has lived with dementia for more than half a decade after diagnosis. While I understand that 40% of USA voters will find the content WRONG because it is very liberal rather than very conservative, I do propose the hypothesis that developing a fairly complex, fact-based mind map of current news shows the value of mind mapping for someone with dementia basing this conclusion only on my own experience. And it works no matter what you think about Trump.
I hope that as many conservatives as liberals will use these methods to study the facts of issues and their own conclusions and evaluate the completeness of what they know.
Examine your memories and conclusions in mind models. Political leanings and party do not matter because your mind model is for YOU as much as my mind model is for ME.
Should you find my political points to be in error, just use this as a template about what you would like to say about, for example, Hillary Clinton or a Democrat in Congress.
But remember that models like the one can be developed by a person living with dementia like me.
And most importantly, I hope that we — whether your political views are similar or dissimilar to mine — can come to an agreement that cognitive methods for supporting thinking for those with or at risk for dementia belong in the next version of ObamaCare or TrumpCare along with training, support, and respite services for unpaid dementia caregivers and especially COVERAGE OF COMPREHENSIVE HEALTHCARE FOR ALL AMERICANS.
Click on the image to expand it.

Oh … and let’s make sure that no President of any party ever uses the nuclear option. I hope we can all agree on that.
The title of this post is the #1 question (comment) I receive on Twitter when I make a post about content on this site.
The answer to the question is a guarded yes. Most (in excess of 85%) cover basic issues in caregiving, healthcare, patient management, note-taking, self description, cognitive issues, case management, family management, and resources within the healthcare system. Some is specific to dementia (mind maps on types, treatments, research, experiences of those with dementia).
My expertise, research and personal interests, and personal theories derive from within the context of dementia in terms of my professional interests, experience as a caregiver for my mother and grandfather, research, test development and personal experiences. So I always present my ideas targeted toward persons living with dementia, their caregivers and medical providers, dementia care/case managers, and those adults concerned with improving and or maintaining their own cognitive skills or preparing for cognitive decline.
There are many applications of my ideas to many chronic and acute healthcare conditions. Caregiving issues are in many cases the same, healthcare management of different conditions may be fairly similar, and nobody has enough resources to do what they actually want to do.
Where I have great reservations in applying (or extending) my ideas about cognitive skills and quality of life is in understanding and intervening in cognitive and the other medical, and mental health issues of children and adolescents. ADHD, adolescent suicide prevention, youthful problem behaviors, dyslexia, and many other conditions require very specialized professional training. Caregiving by family members and paid trained-paid caregivers often requires different skills, knowledge, and emotional supports than it may for adult patients. While many trivialize the issues and state that declining older adults are like children, such a statement makes minimizes (in a way both pathetic and potentially dangers) the very real and large differences in the care of these groups at either end of the age spectrum.
NO posts or mind models in this blog are specialized for the very real unique needs of children, adolescents, and sometimes younger adults.
Click on the image to expand.

I was old enough to vote in my first presidential election in 1972 when I was 21 years old. I voted Democratic then and since then I have always voted for the Democratic candidate often as a perceived lesser of two evils. I voted for Hillary Clinton last year not because she was a good candidate or a good person (in my judgment) but she was better than Mr Trump who was the most extreme political presidential candidate since George Wallace and the most “out of it” candidate since Ross Perot. Before I could vote, I lived through the presidencies of Eisenhower, Kennedy, Johnson, and Nixon’s first term.
I have a neurodegenerative condition that makes me almost uncontrollably anxious at times, obsessive-compulsive at others, and not particular good at decision making. But more than ever, I think that Trump’s Fake Populism is a horrible way to run the USA and the World and I am pretty sure that in spite of cognitive decline my perceptions of Trump are accurate.
Trump’s behavior makes me very anxious and deeply concerned about the USA I will be leaving behind soon. A lot of Americans (according to recent polls, the majority) share my concerns that Trump is an extremely bad President.
I would personally feel much better if the USA required its presidential candidates to take non-partisan medical, neuropsychological, and psychological evaluations before assuming office and annually. My belief is that a group of actively practicing medical doctors enlisted in the Uniformed Services of the United States could make an overall assessment of an individual’s fitness to be “the most powerful person on earth” and commander in chief of the world’s largest army and largest biggest nuclear arsenal, as well as the architect and steward of the world’s largest budget. I note that medical doctors and other healthcare professionals in the US Uniformed Services have sworn an oath to uphold the Constitution of the United States. It is reasonable to expect that the medical practitioners of the United States Uniformed Services can use due diligence and state-of-the-art medical skills to ensure that an individual honored with the duties of the President of the United States is physically and mentally fit to deal with the stresses of the job. I also note that 14 members of the 115th US Congress (2017-2019) are physicians (and 2 are Democrats while 12 are Republicans) and that I have confidence that their medical ethics and competence in medicine would permit a nonpartisan panel to oversee such an assessment (even though I vote as a very liberal Democrat). Perhaps Mr Trump has a medical condition affecting his ability to perform the duties of his office or perhaps he is just a bigoted, narcissistic, incompetent jerk who is quite successful at manipulating the voters of the USA, even without the assistance of Mr Putin and his hackers.
Is my cognitive decline causing my perceptions to slip in their accuracy or are my observations accurate descriptions of living for several months in #TrumpWorld?
Click on the image to expand.

Note. None of the 14 physicians in the current Congress has formal training in neurology. Since a neurological assessment is an important part of a medical exam for a 70-year old person, independent neurologists of either political party should also be part of a supervisory and assessment panel.
Want information you created or curated to have the greatest impact? Then put it into a mind map. Not a mono-toned mess of straight lines at right angles but curves with colors and an organic style. A mind map utilizing rules that follow what is fairly well known about visual thinking. A mind map like the one below.
Click on the image to expand it.

NOTE: Version 11 OF iMindMap was released the first week of May 2018. At this time (7-1-18) I have been using the program for about two months. I will have a full review posted within a week or two. As a brief note, Version 11 includes a number of enhancements. The program remains the best one for mind mapping and the updates made from Version 10 to 11 are significant and worth the upgrade price.
I doubt that there are many people expert in mind mapping who would disagree with me that iMindMap is the most feature-laden of the more than 100 programs for mind mapping to be found all over the Internet.
Once a year — as promised when the program was first introduced — iMindMap has a new release that provides many new features and usability enhancements. And unlike others, they produce a great upgrade every year on time. And free from most bugs that live in Cupertino and Redmond.
How good is iMindMap 10?
Click on the mind map (actually mind model in my terminology) below to expand its size. For those of you with no patience or dramatic sense of the big build-up, you can skip directly to the “9” branch. iMindMap is the 8,000-pound gorilla.
As a note, my review was conducted about six weeks after receiving the program and using it exclusively rather than earlier editions. I use a Mac only, and my review was conducted on a 2013 MacBook Pro. I have worked with the program both on an internal 15″ retina MacBook screen and a 27″ external monitor. [I actually like using the MacBook screen rather than the larger desktop monitor.]

Chris Griffiths and his team at OpenGenius have taken the work of Tony Buzan and in the process of developing a program expanded and formalized that conception in a creative way that is brilliant in its overall utility and ease of use. iMindMap 10 is my favorite mind mapping program, but most importantly my favorite and most useful thinking tool. For those of you who do not follow my blog in general, I live with Frontotemporal Dementia and iMindMap has served as a “brain assistance tool” for me since 2010 in daily living and in continuing my professional interests in a creative way. I can accurately say that the various versions of this program “changed my life.”
This is a tool formulated by expensive consultants who want to help corporations make more money while at the same profiting from that help. But the tool has come to greatly exceed the original vision and is intuitive to use and most adults and all children can learn to use the program for free using Internet trainings. Don’t be scared off by all of the publicity about a $3500 training and a certificate signed by a consulting firm (not an accredited educational institution). You do not need a course to learn this program and it is not clear to me that expensive courses help you learn to apply this program in the real world. If you are willing to invest a few hours you can be doing adequate mind maps; if you invest 10-20 hours you can be doing accomplished mind maps.
Get over the hype and realize that you CAN learn this program quickly on your own and even more rapidly if you study examples available without cost at many blogs including this one (Hubaisms.com), a depository of many thousands of mind maps at Biggerplate.com, and many other sites including youtube.com where many training sessions are presented.
While there are four “views” in this program, the primary mind mapping module is the reason for using this program. The other three views are largely alternate ways of looking at the same information and data. While they may be “quicker” ways to collect information together from a lecture or library research, at the end they feed their data into the mind mapping module where the actual thinking work, theory building, model development, and communication is done.
I have a few criticisms of the program, but these criticisms do NOT change my overall rating of the program as A+.
In summary, this is an amazing program that is much more than a program for mind mapping. It is unsurpassed among mind mapping programs. Additionally it is what I call a “visual thinking environment” or VITHEN. My “criticisms” are minor and do not in anyway diminish my overall evaluation of the quality of the program.
My blog at Hubaisms.com on which you are reading this review was designed and “written” largely in “iMindMap.” Most of the mind maps I use to guide my own “complicated” life were developed in iMindMap.
Exemplary job folks at OpenGenius. Version 10 is an additional large step in the evolution of the program and mind modeling.
Click on the image to expand it.
For those of you who think that the term Dementia Monster is insensitive, do remember that I have one who lives inside of me. Increase my anxiety levels and out he comes. I spend much of my energy trying to limit his ability to feed on the anxiety.

The mind model (aka mind map) below discusses my vision in developing the dementia focus on this website. I started to build the web site about two years after being diagnosed with a neurodegenerative condition (2012). Thus the entire blog is the work of a developer experiencing dementia while designing and preparing the content for the site. The site discusses my progression through cognitive impairment and decline into dementia. More importantly it discusses how I tried to help myself coordinate and use to full advantage the support and professional expertise made available to me by family, friends, the community, my doctors, and the general world-wide of patients and professionals the major issues.
Nothing in this blog post (or any other on blog post or page on the site) is intended to be, or promoted as medical, psychological, or any other form of treatment. The ideas in this blog are about using some commonsense note-taking and visual thinking methods to possible help you live better with dementia. I tried it on myself (only) and I am encouraged although I freely admit that full scientific study is needed.
These methods and comments will not substitute for medical and other professional treatments. They do not cure dementia. They do not slow down the progress of dementia. For me, at least, the methods have sustained and increased my quality of life and I do spend more time with my family and am more independent and in my opinion think better. But my dementia is not being treated and getting better; what I propose are methods that may make it easier to independently manage selected parts of your life, be in a better mood because you are trying to help yourself, be less of a burden to your caregivers, and report better to doctor what your experiences have been since the last appointment.
Many people are miserable almost all days when they have dementia. If simple, inexpensive cognitive tools can improve some or many of those days, the development of such techniques is a huge step forward.
I hope that others will examine the information here and use it to improve the decisions they, their caregivers, and their doctors and nurses must make about their formal medical treatment.
Here is what appears in the blog posts and elsewhere on Hubaisms.com.
Click on the image to expand it.
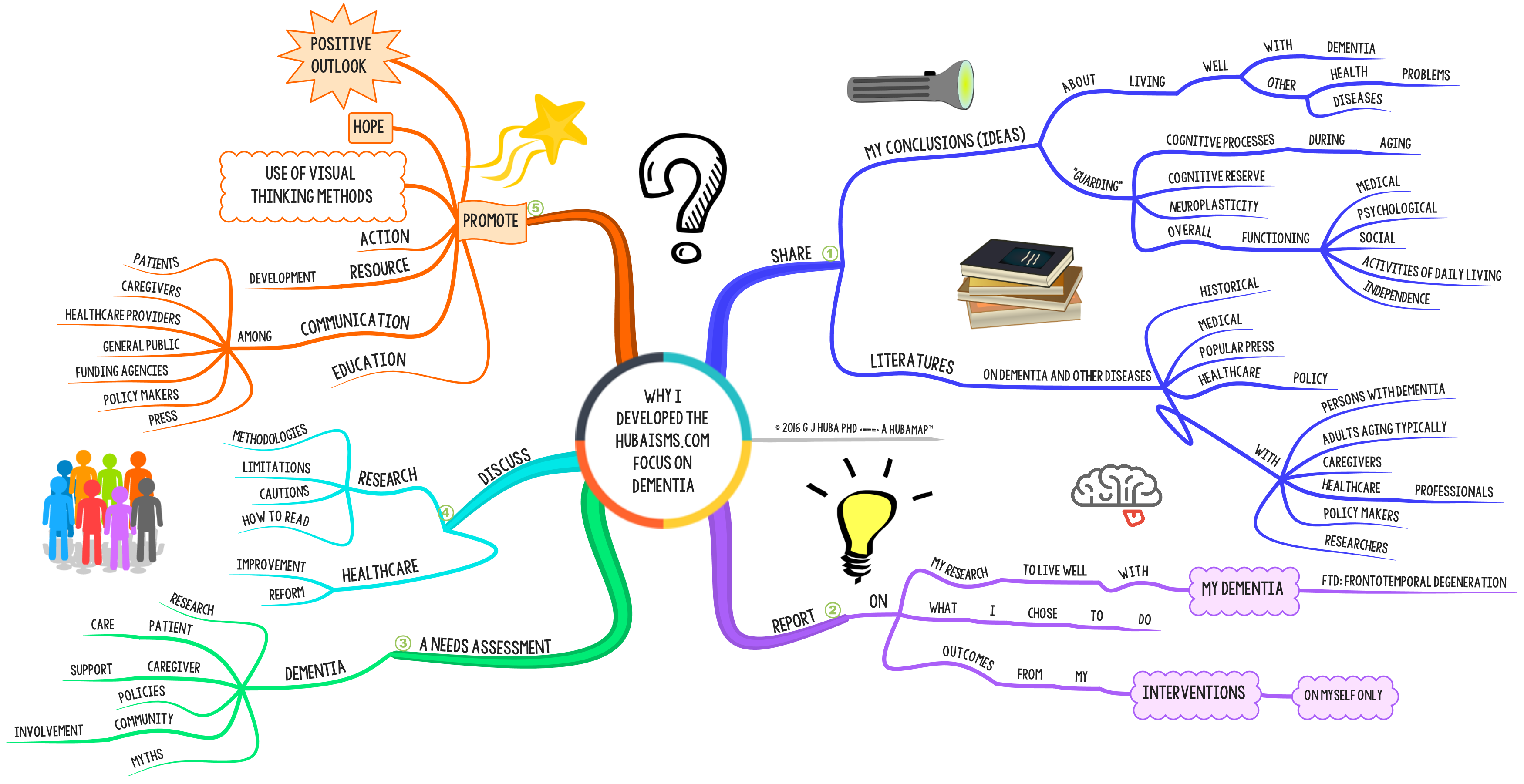
Click here to see Part 2 of My Vision in a separate window.
Not the past, not what might happen in the future. Fuzzy, intuitive, today’s emotions. Nonlinear, visual, big picture. Attention flows toward good, bright, happy visualizations.

Opening your mind to nonlinear thinking may provide a cognitive reserve that helps you as cognitive functions start to decline perhaps precipitously into dementia. Neuroplasticity is a mechanism that the brain will use to reassign functional processing from one area to the brain as it is damaged by trauma or disease.
One very good way to encourage the development of cognitive reserve and neuroplasticity is to practice nonlinear thinking methods that can help promote mindful solutions. Should the brain become damaged, it may be able to use nonlinear, symbolic visual thinking to cope, at least for a while. And while you practice you may also experience strength in your resolve and understanding.
Do note that the above comments are speculative. There is NO formal research on mind mapping or other comments about this in the literature (other than my own). Also, this is based only on my own experience and generalizations from my earlier research on daydreaming and imagery. So do not go about thinking that this proven. Rather it is speculative.
While I theorize that mind mapping is related to mindfulness in SOME applications, even if it turns out that it is not — from the results of formal empirical studies — there are other demonstrated benefits from mind mapping, so the actual use of mind mapping should still be encouraged.
One way that healthcare communication can be made more effective is to supplement or replace traditional pages of small-type textual information with graphic displays such as mind models (AKA mind maps), sketches, graphs, and infographics.
This post focuses on mind models (mind maps). The same general arguments would apply to sketches, graphics, infographics, and other visual information methods designed to promote a more effective patient-oriented healthcare system with more complete, accurate, and easy-to-understand information for all.
If you are not familiar with mind models (mind maps), you should look at the mind map at the bottom of the page first (Footnote).
To expand the graphics, click on the images.

Footnote
There are many problems that can plague a person with dementia. Some of these are easily detected but others may be “hidden” because of the nature of the major symptoms of the disease or “hidden” because the person with dementia (or caregiver or in some cases family members) is trying to hide some of the problems from outside observers.
For instance physical, psychological, or financial abuse will be hidden by the abuser and perhaps the person with dementia. Memory loss may make it difficult for the person with dementia to accurately report accidents.
It is important that healthcare providers, caregivers, and family members be trained to identify the hidden problems.
To some degree or another, it is likely that most persons with dementia have some of these hidden problems. For instance, I bump against things all day long, usually because I am rushing around or not paying attention because I am trying to multitask. When asked by a family member or friend where the bruise came from, I have to try to reconstruct where the accident must have happened by thinking through a lot of alternatives for a bruise half-way between my ankle and knee.
Click image to expand.

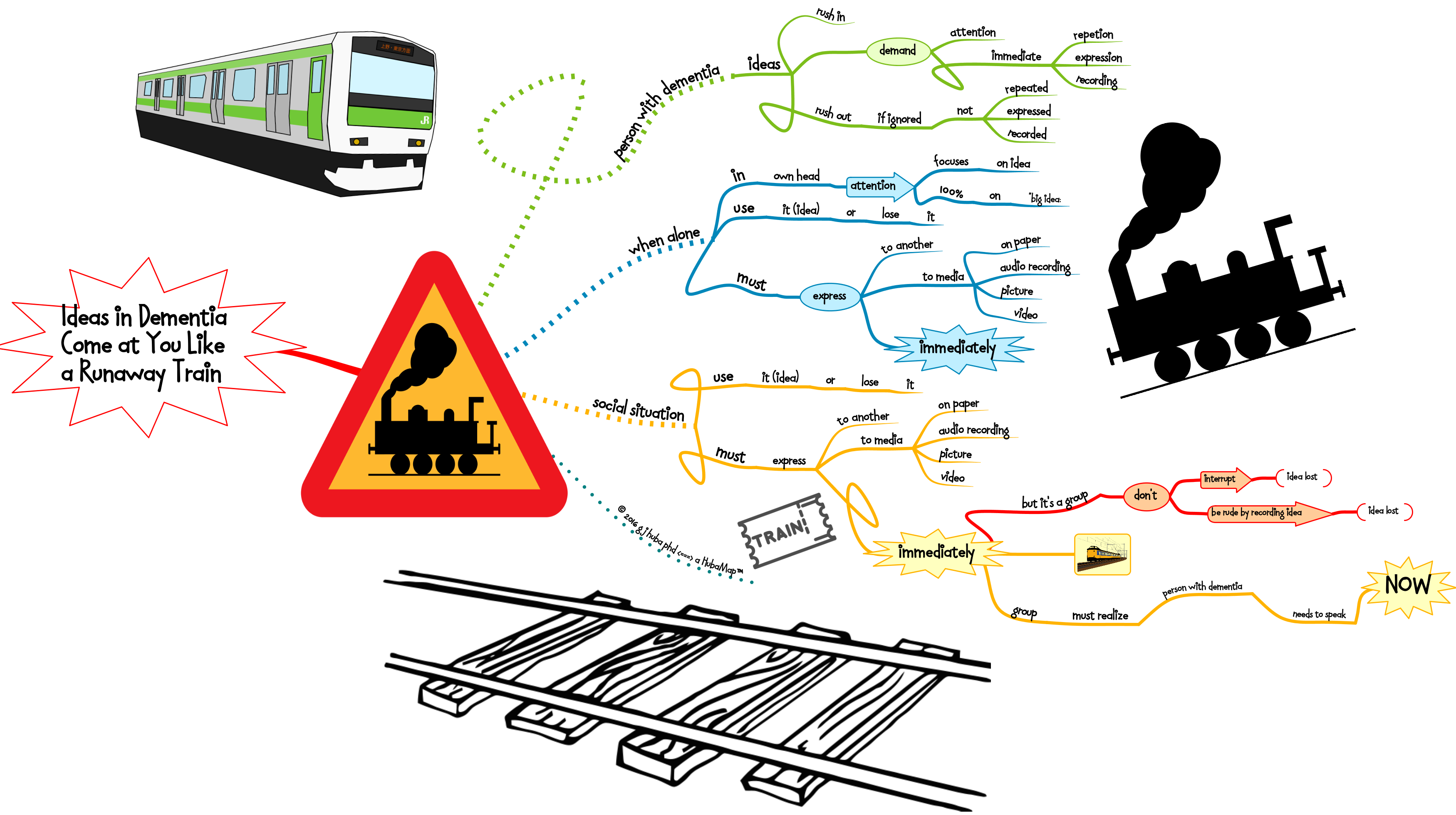
A mind model (aka mind map) on the way that ideas hit you when you have dementia.
In a group, the need to say something immediately before you forget it often takes a backseat to etiquette rules of waiting for your turn to say something and not interrupting. If you are talking to someone with dementia, consider cutting them slack and letting them jump in when they can. If the group won’t let the person with dementia break in it can lead to both a sense of frustration for all and quite frankly, the loss of some good ideas and interactions.
The current rules of etiquette do not take account of the fact that some of the participants in an interaction will have severe cognitive impairment or mental illness that pretty means that if a thought is not expressed immediately it will be forgotten.
Sometimes rules need to be stretched or curved (like a railway track) and patience exercised. This is one of those times.
f I am trying to blurt out an idea to you, believe me that if I don’t say it immediately it is going down the track far, far away from me. And it may not come back for another five minutes (if at all).
Click on the image to expand.

I have been a HUGE fan of the Olympics since I was a very little kid. In 1984 I got to go to the Olympic events in Los Angeles every day for two weeks, on many days with my father. That was the year that the Soviet Union boycotted the games because the USA had boycotted the Moscow Olympics in 1980. Heck, I thought it was great — the USA and East Germany (who came) won all of the gold medals! Months earlier when local pundits in Los Angeles said Los Angelenos were too apathetic to purchase expensive Olympic tickets especially with the Soviets and most of the Eastern Bloc boycotting as it would not be a real sporting event, I had bought as many tickets for the “finals” as I could get my hands on. Later I sold the extra tickets as Los Angeles fell in love with the games. I made so much money that the expensive tickets I had bought for the entire family of 7 that we used ended up were effectively free since the profits covered the cost of the tickets we used. Street enterprise at its best. My tickets became worth more because the Soviets didn’t come as all Americans became Olympic fans the year we won all the golds.
Winning the race to live well with dementia is like running the 10K race at the Olympics. Everybody has to pace themselves at the beginning so that they can learn about their opponents. In the final stages of the race they speed up and sprint their fasted the last 200 meters.
A mind model of the dementia race strategy is shown below. Click the image to expand it.
I think I am winning my race to live life to its fullest while having dementia. I’m getting ready to claim that gold medal. You can win your race too. Think about what you are doing and strategize like a 10K runner. Learn all you can in the beginning and then speed up later as your new knowledge kicks in.


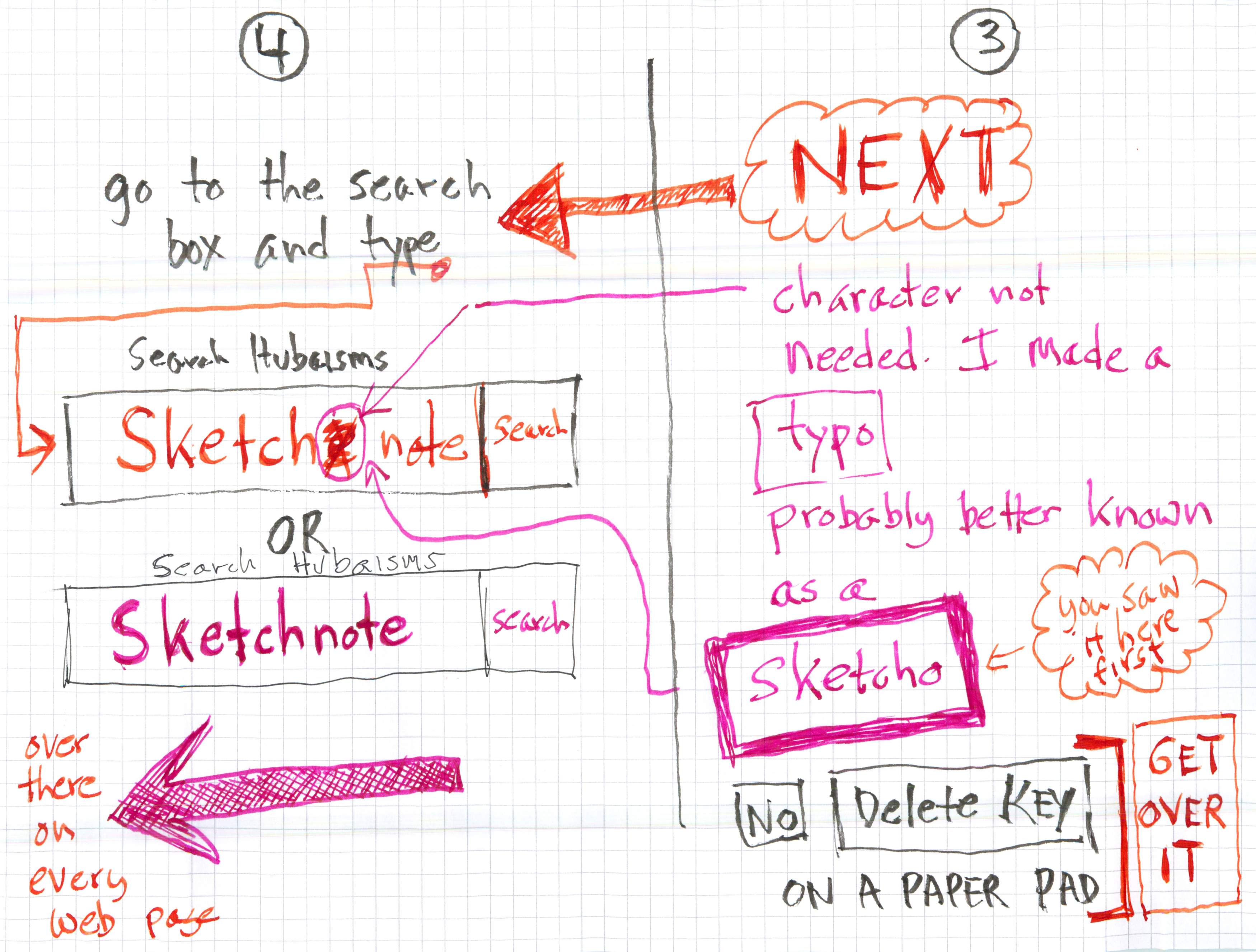
I expect to be adding a lot of posts about (or using) sketchnotes in the next few months to Hubaisms.com. Here is how to find the existing ones and the ones I will add. The information as a sketchnote. Click on the images to expand them.

The politicans made me do it …
Click to expand.


Click on image to expand. Estimated time to develop for a NOVICE (me) = 15 minutes. The sketchnote was drawn by a person with dementia (me).
[Note. I usually write/draw note panels like this from right to left in sections because I am left-handed and it minimizes the amount of smeared ink. There is no magic in this, so use any organization that works for you.]

Ever wonder what the difference is between Mind Map techniques developed by Buzan and Mind Model theory and techniques developed by me?
Probably not.
At any rate, just in case you have an itch to figure out the difference later, here is a cheat sheet in a Mind Model. Click on the image to expand it.

Did that get rid of the itch?
There are 5 basic choices, although more than 1 option could be executed simultaneously. For instance, one well-recognized American wanna-be POTUS would use options 1 and 2. One liberal blogger would combine Choice 5 (most important) with Choice 4.
Click on the image to expand it.

In the long run, Choice 5 will work best. Choice 4 eventually needs to be done no matter which other choices are made. Choices 1-3 are merely band-aids at best, and demagoguery during an election year in the worse case.





























