No covid vaccine yet. Even if one were to be fully tested and proven safe and effective tomorrow, you probably could not get a shot until 6-9 months later.
Mask use seems to be topping out at around 70% in the United States and even conscientious mask wearer and social distancers are getting pandemic fatigue and less conscientious about always using protective behaviors.
The USA is not using behavior change and social support methods to help deal with unhealthy and potentially virus-spreading behaviors.
Instead of promising a vaccine and telling me to wear a mask, how about some social support methods to help with people feeling the depression and anxiety and hopelessness and fatigue and loneliness that comes during a pandemic. Most Americans could use some support in dealing with the balance between working and providing childcare/homeschooling. Or the frustration of being alone at Thanksgiving.
How about promoting behavior change and showing people how to get a mask to fit comfortably and correctly, or showing people how to judge they are six feet away from others. How about getting cigarette smokers to stand 12 feet away from others as they do the huffing and puffing thing in service to nicotine addiction.
A lot of people would benefit from counseling and group support-self help groups during a pandemic.
Many need a case manager to help them get food or a place to live or a job or child care or eviction or mortgage default. Others may need a legal counselor to help deal with problems incurred because of wholesale job loss and the resultant loss of life savings.
To stop the spread of COVID-19 you cannot just tell someone to wear a mask or not go to a family member for support.
What you need to do is to help individuals with pandemic fatigue and other problems find ways to constructively deal with the pandemic and get help from public sources.
Fortunately, most of the social services needed to help many people deal better with the pandemic can be provided by trained mental health and healthcare professionals and their assistants. When provided by telephone or video sessions or online support groups and counseling or specific advice to someone getting evicted these services are much less expensive than treating someone in the hospital or outpatient clinic who has become infected with COVID-19. And of course, every person who gets COVID-19 can potentially die or be affected by lingering symptoms for the rest of their lives, and the cost of any life or development of a lifetime disability is one we should try to avoid as completely as possible.
If we want to cut the levels of COVID-19 we need to up the prevention, support, and behavior change services we provide.
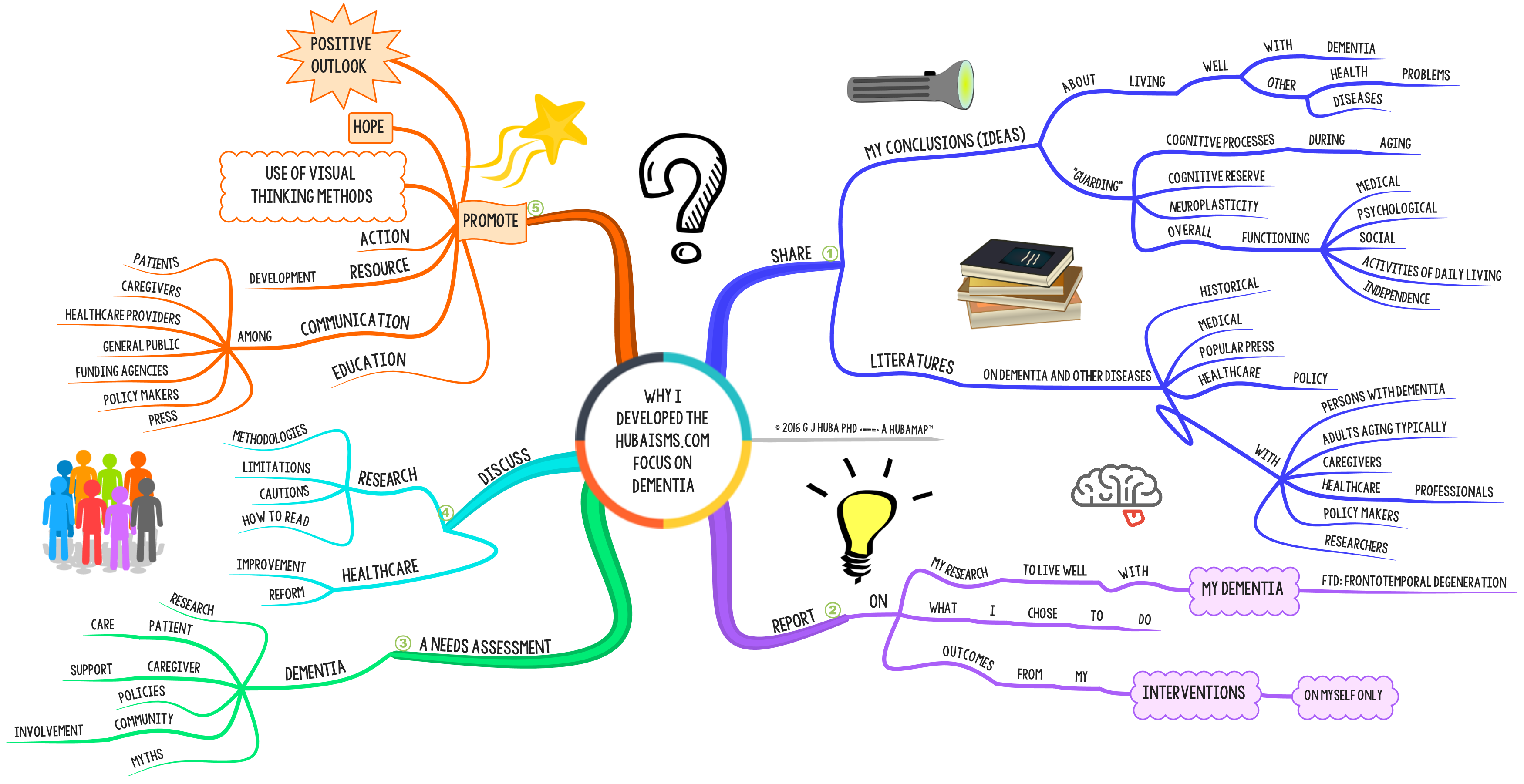
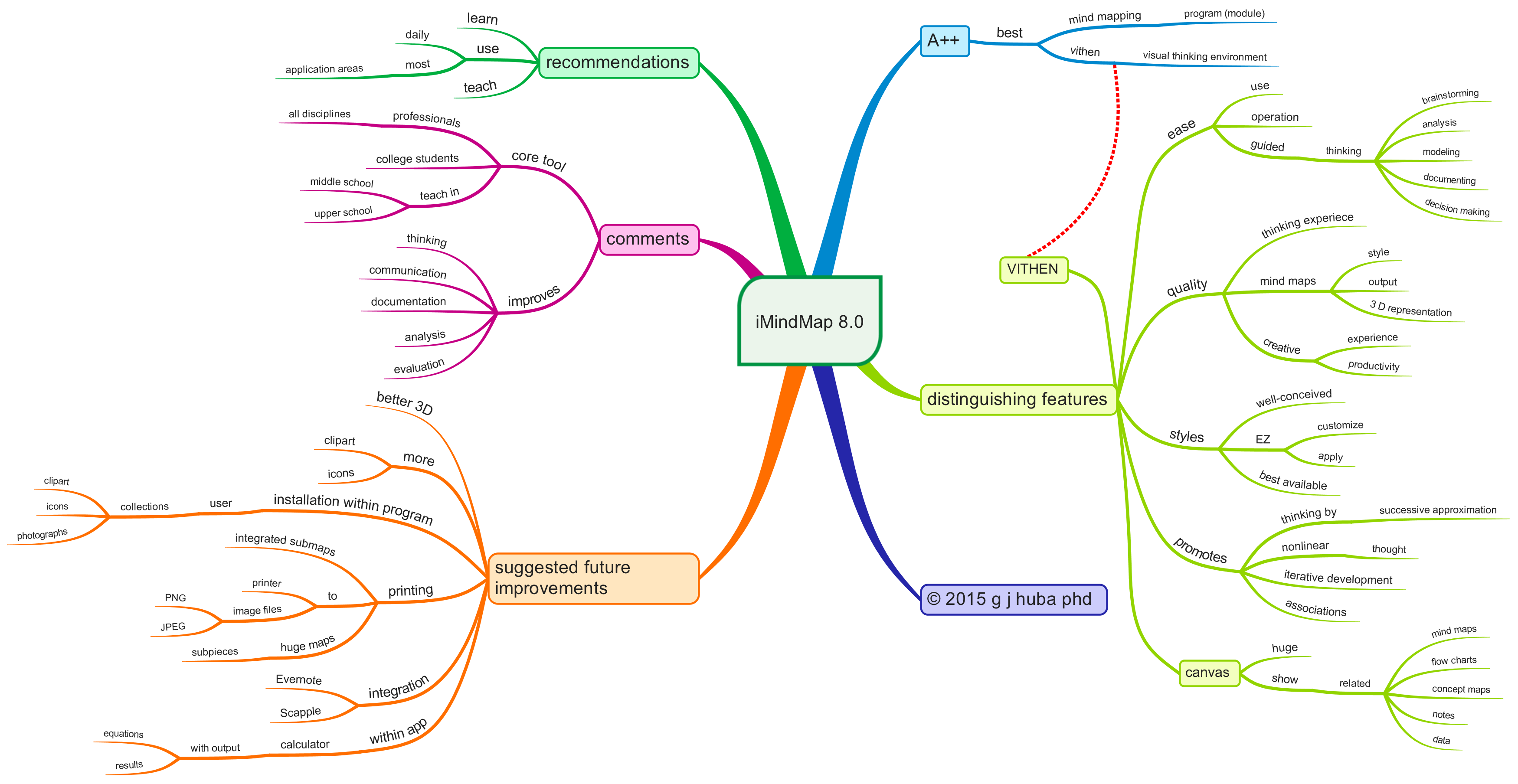
Click on the mind map to expand it and look at the issues in providing behavioral and support services that could make it easier for people to avoid dangerous behaviors that spread the disease.
![]()



































![mindmodel™ [mind model] 2016 © g j huba phd](https://hubaisms.com/wp-content/uploads/2016/05/mindmodele284a2-mind-model-2016-c2a9-g-j-huba-phd.png)






































{kind=link}
{kind=link}
{kind=link}
{kind=link}