and don’t walk out until you understand the answers.

social, health, political imagery through the lens of G J Huba PhD © 2012-2021
and don’t walk out until you understand the answers.
Since the 1960s, the US Congress has borrowed money from the Medicare and Social Security Trusts — money deducted from the salaries of all workers — and used it for defense, foreign aid, defense, social services, defense, medical services, wars, defense, bombs, and Congressional pork.
Now, Trusts funded by by workers’ salary deductions to pay for retirement living and healthcare expenses are supposedly going to go bankrupt because dementia is reportedly going to destroy these programs.
Truly one of the great cons in history. For decades Congress has committed fraud by stealing from the pension fund Trusts to pay for goodies for special interests that have resulted in their own re-elections.
Now, instead of getting mad at Congress and throwing the big violators in prison, we (or my children) are supposed to get angry at our parents for having dementia.
The US has prosecuted organized crime for decades for stealing from pension plans.
Somehow we forgot to prosecute the biggest violator.
Stop blaming dementia for the destruction of Social Security and Medicare. Responsible elected officials would not have stolen from these trusts or would not have enacted tax cuts while taking money from needed social network services from the future.
There is a way to fix this problem available to you in November. I hope you use it.


The experience of time when you have dementia is quite different from the period before you had dementia.
For me, one of the larger changes that occurred is the experience of time, both in the short term (during a single day) and in weeks, months, and years. Compressed yes. Also VERY NONLINEAR.
Here are a few suggested names I have come up with for the time zone in which many persons with dementia live.
There are two big problems in this naming process.
First, there are many different experiences of time so not all persons with dementia are “synchronized.”
Second, persons with dementia can live in more than one time zone simultaneously. I am a good example of that. I think of this time zone shifting as being in a science fiction novel going through alternate universes in a time machine. Dr. Who on dementia.
Never one to walk away from a challenge …

Ok, I may not remember your name unless I knew you years ago. I get confused when people speak to me, especially in loud and noisy settings or when I miss a word or two and cannot “fill it in from my archival storage.” My spelling is getting bad and my words shorter, although I will point out that I have spelled stoopid intentionally incorrectly for more than a decade. I tend to avoid social situations not only because they are confusing and I cannot screen simultaneous conversations from one another and have no awareness of either my tone or volume of voice and thus may decline an opportunity to go to a reception at the White House next week which for me would be a once in a lifetime event. I can usually spell arithmetic, but sometimes not; I probably look up the spelling of 50-100 words per day on Google when I am answering email or blogging or tweeting, but somedays I can spell a word and later not be able to spell the same word. I tweet dozens of times a day to 100,000+ followers but have to look up all but a dozen twitter IDs if I want to send a message to an individual. I do these incredibly complicated mind maps to make my ideas accessible to more than I could using words. I do not remember when TV programs I have liked for years air but have solved that problem with a DVR. And a lot of people who have to interact with me each day think I am dumb or slow or stupid and show it in their behavior toward me. Others are quite kind and understanding.
How do you think the the ones who think I am slow or dumb or stupid would react if I said, “I’m not stupid, damn it. I just have dementia.”
Think about that.
I’m not stupid, damn it. I just have dementia.
AND I HAVE ADJUSTED TO DEMENTIA IN MANY WAYS.
Let me repeat the whole message.
I’m not stupid, damn it. I just have dementia. AND I HAVE ADJUSTED TO DEMENTIA IN MANY WAYS.
Don’t treat others whose behaviors are “odd” or are judged by observers to “have Alzheimer’s” or another dementia as if they were dumb or stupid. Many are quite aware of at least of part of the behavior around them but may not express emotions nonverbally anymore or gaze at you while you are talking or respond in the words you expect.
They are not stupid, damn it. They just have dementia. And many adjust to dementia in many ways.
I was smart enough to put “darn” in the title to this post rather than “damn” as I suspect many of you find the euphemism more acceptable and my preferred original wording disrespectful. I personally use the phrase “damn it” to honor my grandfather, a proud New Englander who hailed from Vermont. Sort of like Bernie Sanders without Bernie’s tremendous social enlightenment (it was a different time when ignorance became bigotry and he had little religious tolerance but no racial intolerance at all and was a proud unionist).
I have a PhD degree from one of the best universities in the world and even though that does not guarantee I am not dumb or incredibly stoopid, it was necessary to be able to spell and speak coherently and add simple numbers and do fourth grade word problems in order to get the degree. I used to be able to remember hundreds of phone numbers and never had to carry an address book. Now I may not remember to call you back. But I am still aware enough to say to Siri or Alexa “what is 4227 – 3101” after I use a calculator to check myself and my fingers. And I hate any computer program that does not have a built-in spell checker. I need that spell checker a lot and it is not because my fingers do not work well.
I’m not stupid, damn it. I just have dementia. And I adjust to dementia in many ways.
I am quite aware that people respect me because of my writings on social media (although they may think I am a jerk because I espouse too many liberal causes, believe in letting Syrians and any others practicing Islam or those from Middle East origins into the USA just like any other people, and thinking a Trump presidency would be a coronation and disaster). People on the street may not see me as much more than a prematurely old-looking man, not always well-dressed and freshly shaved, walking looking down so as not to fall, and who asks you to repeat many sentences because he does not understand you the third time you say something.
I am spending more time now at a local community that features in-home and multistage assisted living of various kinds. Sometime soon I will move in there because it is time, although I do not need much assistance now nor should I for a while. At lunch and walking around I see lots of people who cannot figure out the lunch menu at times (I am included) but can discuss their former high profile careers (many were university professors at UNC and Duke), the looniness of Donald Trump, and favorite classical composers while not knowing how to get somewhere across town. Tomorrow they may not remember my name or the conversation (I forget names but remember conversations) we had yesterday until at some time they say, “Oh you were the guy I was talking to about the UNC basketball game when we were here yesterday.” And, although Donald Trump seems to be quite a topic of conversation at times (usually in proximity of a television set when CNN is on) among those I identify as having significant cognitive impairment/dementia, I have yet to hear a single person say anything nice about the man. Certain types of wisdom seem to stay with you.
They are not stupid, damn it. They just have dementia. And they adjust to dementia in many ways.
We are not stupid, damn it. We just have dementia. And we adjust to dementia in many ways.
A few thoughts in a mind map. Click on the image to expand it.

The presentation below is an alternate way of display the mind map above. A few portions of the mind map are shown at a time. The presentation will run automatically or click the pause button in the presentation and use the arrow keys to go back and forth manually.
My grandfather lived to be 87. He had dementia for at least the last 10-15 years, probably longer. He never failed to light up in a smile and he never heard a baseball game on the radio (or watched on TV) that he could not understand. And heck, right until the end, he never voted for a Republican.
He wasn’t stupid, damn it. He just had dementia. But he knew which political party would treat regular guys who served in WWI fairly and in spite of battling dementia and not smiling much any more, at the age of 84 had my mother help him buy a new suit and insisted on coming to my PhD graduation. Later that day during a moment of lucidity, he told me his family had progressed from the first one to graduate from high school (him) to the first one to graduate from college and a masters’ program (my Dad), and now me. He always loved the USA and democracy above everything and was proud his family had made it in his beloved country. And to the day he died, if there was a Red Sox game on the radio, he was listening to it. And understanding it. And always rooting for any team playing the New York Yankees, something he had learned to do way back in the days when professional baseball was just starting.
Oh, and before you say that this post is too well written to have been done by someone with many cognitive deficits, take into account that I worked on it for more than a week and wrote from a number of mind maps and other diagrams. I have been thinking about these ideas for several years and I went through more than a dozen drafts, often writing just a few sentences at a time.
I adjust. Please try to adjust to that old man who bends over and looks at the sidewalk when he walks, may not care about coordinating clothing as it takes him back to his youth in the late 1960s to be uniquely dressed, and does not necessarily shave until after lunch because it is much easier to use a razor or shaver at the times of the day when his hands have less tremor.
If everyone adjusts just a little more to people with dementia and people with dementia try hard to adjust a little more as they decline, we will have communities that become dementia friendly naturally. And guess what? Dementia-friendly communities will be less of a burden to taxpayers because people who can continue to live in communities at least semi-autonomously do not need as much caregiver attention or healthcare. Think about that carefully. Help create a community easier for people with dementia to navigate, make them happier, lower taxes, and make your friends and neighbors who are family caregivers a little more relaxed. Who could argue against such a plan?
Certainly not me or the volunteers throughout the world working hard to have dementia-friendly communities.
I do. Thanks to lots of help and love and caring from many.
As I discuss throughout this blog, there are many things a person living with dementia can do to try to adjust so as to have a better life. Among those are using different tools to help with changes in memory and other brain functions, adjusting expectations, and establishing different patterns of behavior. Your brain can never return to its pre-disease state but you may be able to improve your quality of life by learning how to write an effective post-it note for reminders, mind map, explain your dementia to others, and plan. These are not treatments but rather ways to adjust so as to cope better. And coping better can improve your quality of life it it means less anxiety-filled time, or extra visits from family and friends, or being semi-independent longer, or shopping for your own groceries and planning meals.

Every little bit helps. Greatly. In maintaining quality of life for as long as possible.
Besides telling you to lose weight, walk as much as possible and not eat various foods with your medications, has you help care provider shown you how to make little adjustments or referred you to another agency or doctor who can do so.
Thought so. Healthcare models that include behavioral and cognitive interventions and refer you to a specialist who can help are few and far between. And your health insurance may have significant deficiencies for reimbursing you for the cost of such services.
Healthcare needs to reassess its vision of goals and working methods to help people who cannot gain much help from traditional pharmaceutical interventions to still achieve a good quality of life. See if your doctor or another healthcare provider can help.
Social workers are a key part of a dementia care team. The following mind maps shows why. Click the image to expand it.


There are 5 basic choices, although more than 1 option could be executed simultaneously. For instance, one well-recognized American wanna-be POTUS would use options 1 and 2. One liberal blogger would combine Choice 5 (most important) with Choice 4.
Click on the image to expand it.

In the long run, Choice 5 will work best. Choice 4 eventually needs to be done no matter which other choices are made. Choices 1-3 are merely band-aids at best, and demagoguery during an election year in the worse case.
Crank up the Jimi and ZZ, Maybelline. Tune-up the Les Pauls and Fenders. And wear your High Heel Sneakers and lots of old denim.
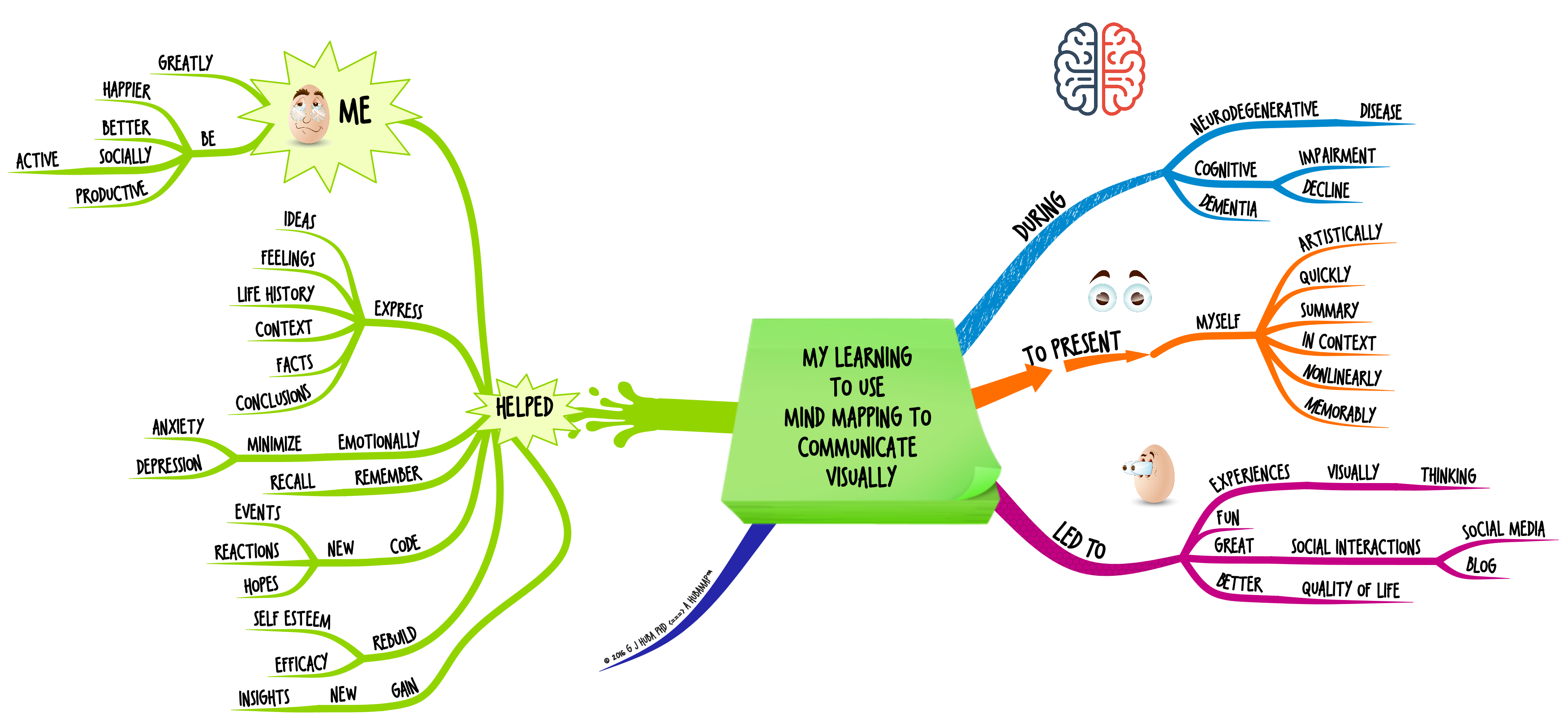
My reasons for developing and using and encouraging mind maps on dementia.
Click image to expand.

Enter a caption
The first dirty little secret of mind mapping is that consultants on mind mapping who know little (or in most cases nothing) about neuroscience and cognitive psychology and dementia will make mind maps with dementia content that is “questionable” or just completely wrong and do not hesitate to share it on the Internet or through other forms of marketing. Many commercial claims such as “discovery” or “research” will be made. But it is very likely that the maps being sold are not valid or relevant and could “hurt” persons with dementia.
The second dirty little secret is that many of the content dementia mind maps are made by computer program developers who just want some colorful maps to sell their programs. These companies do not use current evidence-based research or expert consultants or persons with dementia as a source of information.
The third dirty little secret of mind mapping is it takes years to learn dementia care and a 1-3 days o learn mind mapping to an acceptable level to develop nicely-formated mind maps.
Who do you think is more likely to produce mind maps relevant to the health care system that will not hurt patients by providing poor information? Category 1 or Category 2?
The answer is a no-brainer. If you cannot see the difference between valid information from Category 1 mind mappers and that from Category 2 mind mappers you should not be producing dementia or other health-medical mind maps.
A mind map with the issues follows. Click to expand it.

The following automatic presentation shows the major issues in assessing the value of mind maps offered for sale (or free). It contains identical information to the mind map above but is formatted so as to show one part of the map at a time. If you would like to run the presentation manually, hit the pause button within the presentation and use the arrow keys on your keyboard to work through the presentation at your own pace.
Mind maps are powerful thinking and communication tools. But, especially in the fields of healthcare, social care, medicine, and mental health, mind maps need to reflect established evidence-based research OR clinical observations OR careful observations of persons with a condition and their caregivers. For the professionals, individuals should be licensed by their local jurisdiction as required by law. Patients and caregivers should be receiving treatment and information from physicians or other licensed professionals as part of the person with treatment.
Medical and health mind maps must developed to a much higher standard than business mind maps. In the business arena, the content in mind maps typically is developed from personal theories of individuals and is rarely substantiated by peer-reviewed research, careful observation, and is typically motivated by obtaining and retain consulting clients.
While I personally believe business mind maps should also be developed to a higher standard for their content and theoretical as well as business motives, I KNOW that medical and healthcare mind maps for people with dementia must carefully reflect the experience of the person with dementia, family members, caregivers, clinical observations, and peer-reviewed research.

and knew it could become so, but was not there yet.
Most of the life and care management I wish to do can be voice controlled by my more intelligent assistant Siri. Siri’s ability to capture spoken words and translate them into text is a marvelous assist in guiding my calendar, making notes, finding out television schedules, remembering friends and appointments and phone numbers, autodialing and voice activated texting.
The missing feature that could make the iPhone my real best friend?
“Hey Siri, where are you?” Beep, beep, beep, beep beep, beep beep, beep beep beep beep beep beep beep” to an ever louder, faster, and higher tone. Oh yeah, and flash your screen and start vibrating even if I did not set this in the options.
I bet you would like this feature — A LOT — even if you do not have dementia. If you do have dementia, without this feature you may never see your iPhone again after you put it down.

Click image to expand.
Have dementia? So do I. You and I and others can use Twitter responsibly to provide information and observations and comments to millions of others, any one of whom might use that information to make a difference in treatment systems, the development of pharmaceuticals, priorities for the use of tax dollars, or the care of a family member.
Pssstttt… these techniques are for anyone advocating for just about any social issue. Pick a good topic you know something about and become a One Person Advocacy Organization.
Click on image to expand.
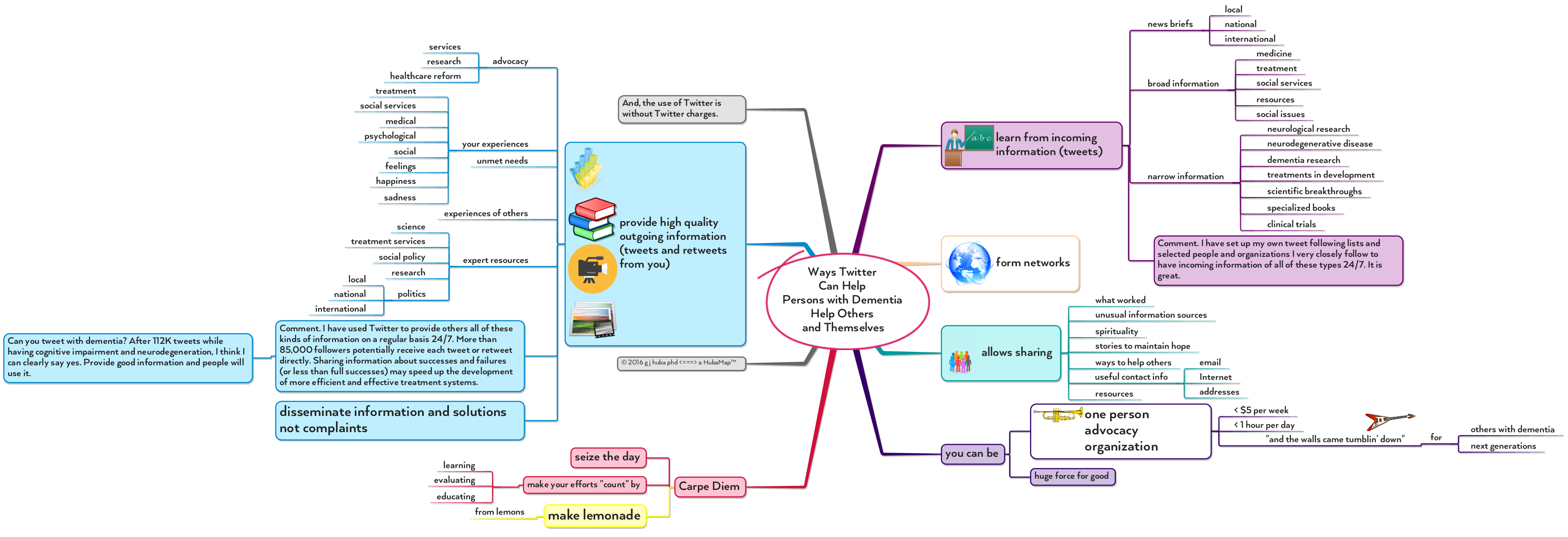

Better non-medical outcomes for person with dementia, low cost to train, low cost for software, huge benefit for the costs … what is there not to like?
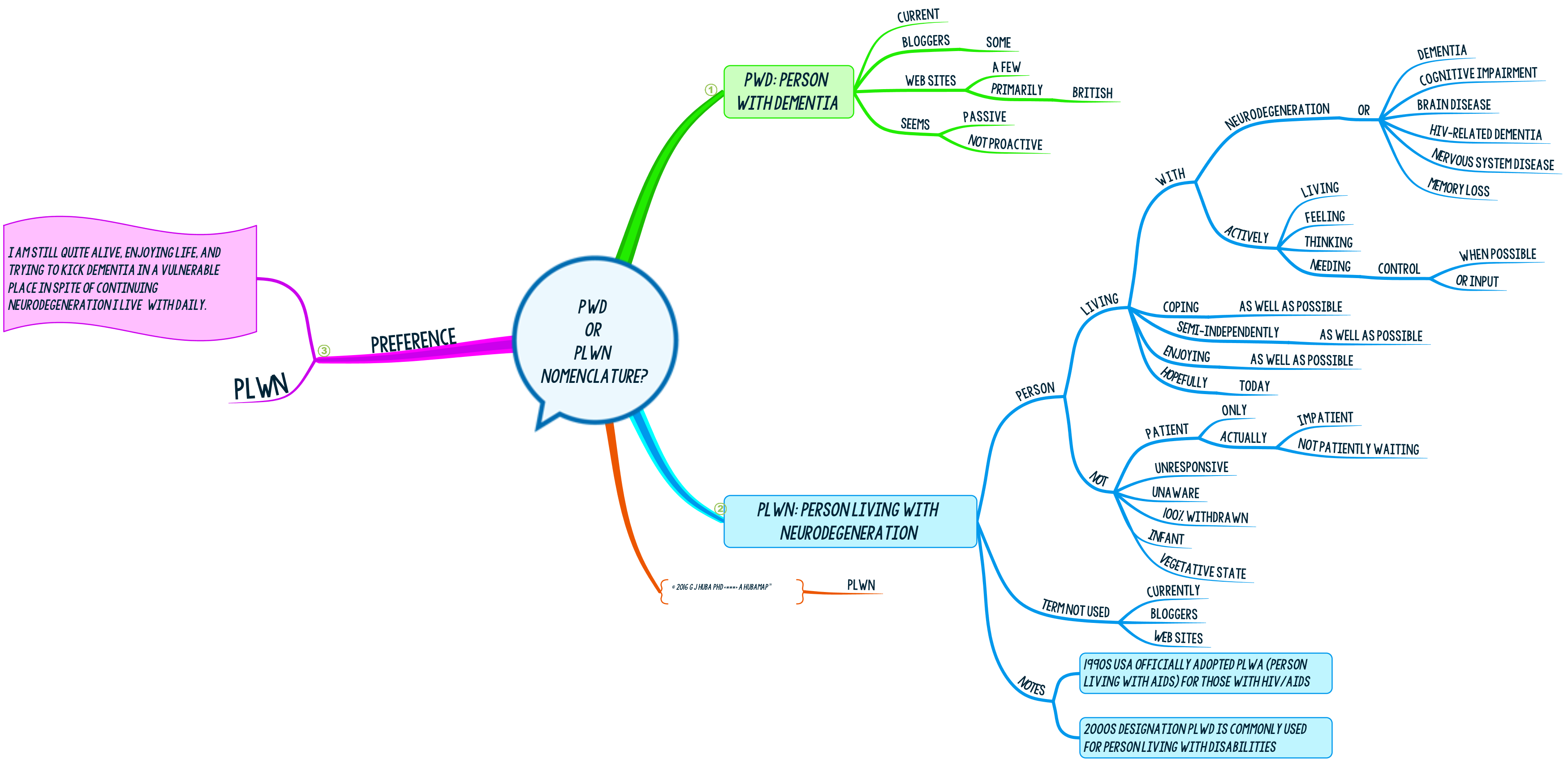
Nomenclature and acronyms greatly influence how we describe and study medical conditions. PWD or Person with Dementia is the current term. I like Person Living with Neurodegeneration or PLWN. Here’s why. On the other hand, PWD will probably still be in use long after I die.
The arguments for PLWN. Click mind map to expand.


Great Visualizations ==> Understanding

I was diagnosed with neurodegenerative disease in 2009.
There is a long-standing tradition in the fields of psychology and medicine of individual (or case) studies in the early stages of studying a disease, a possible treatment, a theory, or basic research studies.
Often these studies are done to open a new field for exploration or to “seed” progress in some new ideas. In psychology, many of the theories of learning and behavior change originated from studies of single or a few individuals. In medicine, most progress starts with a skilled clinician identifying a new symptom or pattern of symptoms and biomarkers or response to a drug in a single or few individuals.
Single individual studies are widely used and considered valid by many. But they are not considered to be valid (by themselves) by the majority of the professional community.
The Number 1 NO-NO in single individual studies is to study yourself. The reasoning goes that one cannot accurately describe oneself. The commonsense part of me says that rejecting such information is STOOPID but the well-trained methodologist in me says to eliminate the possible bias by having an independent party (presumably a physician or psychologist or equally qualified and appropriate professional) conduct the study.
So I ignored my commonsense and asked more than a dozen MDs and PhDs if they would like to take advantage of the fact that I had more than 35 years of experience describing behaviors and feelings and treatments and outcomes and also was taking lots of careful notes as I tried a number of techniques to deal with the disease. Most could have also found out on the Internet that I have hundred of peer-reviewed scientific publications and was myself considered one of the methodology gods. NO takers to date to use my information or expertise. I think all of the people I approached were scared off by what their professional peers, tenure boards, department chairs, journal editors, ethics boards, and the current Methodology Gods might say. Most just ignored the “demented” person and probably felt sorry for me. One proposed that I spend thousands of dollars (which I had lost due to the brain degeneration and its effects on my financial decision making) to come to the other side of the USA so he could examine me (he had lots of grants so I informed him that I knew he would have travel funds in his many projects and that if he wanted to do research on me I would go through the hassle of a 2300 mile one-way trip he could use his research funds to pay for the ticket). After that he never responded to my email.
Although I was ignored by the academics, I took solace from the fact that about 120,000 unique individuals in social media (Twitter, Google+, Scoop.it, Linked) choose to follow my tweets, blogs, and comments. They seem to place some confidence in my judgments and communication skills. I did not disclose that I had dementia until I had about 85,000 followers but I did not dramatically lose followers after I made the announcement. The community of those who follow me is heavily weighted toward medical and healthcare professionals and organizations, psychologists, social workers, persons with dementia, care givers, family members, and mind mappers. Many of the physicians who follow me are neurologists and psychiatrists and I have healthcare followers in more than 100 countries.
So I struck out on my own. As I think about it now, I do wonder if perhaps those who are self-proclaimed independent observers-researchers could, at this time, study a person with neurodegeneration-dementia with their academic and somewhat unreal methodologies and understand the experience of the condition. Having dementia and also being able to think well at least part of the time is not something these folks or the general public “get.” So far as I know, nobody with my level of relevant training and dementia has ever come forward and states that there are a lot of methods you can do to reorganize your thinking. I used them to improve my life and trajectory through the stages of the disease, so far as I can tell. Those without dementia or cognitive impairment cannot understand that while it is a difficult mountain to climb, it is not impossible to reach the summit at least in the earlier stages of neurodegeneration and that the goal is to have a “good and enjoyable life” for as long as possible, not to “cure” the brain with better ways of storing information, keeping notes and reminders, or decision making.
Once when I questioned whether I should share all of the information I present in this blog in front of so many people my neurologist at an appointment told me that if 100,000 people were following me I should not be concerned as at any time they concluded I was wrong they could (and would) unfollow and simply not follow the information I was presenting me. While I would never expect any of my own doctors to follow my blog, she admitted that she “looked in from time to time.”
So I acknowledge to the Methodology Gods that I have sinned but I am not very worried about being thrown in the volcano for the deviation. After all, somebody with neurodegeneration-dementia has to step up and tell the “experts” that experience (in my case the synergy of the professional training and personal history) counts for a lot and and I have used some real data I have carefully collected that they should consider and use to design more studies.
So that’s it. I sinned, I am not contrite about it, and you can judge from what I have written here on my blog whether I am delusional or a thoughtful scientist. My own judgment is that both characterizations are probably true depending upon the day of the week, phase of the moon, whether my dog has been insisting that I go out in the woods with her to chase critters or whether I am suffering that day from the horrible headaches caused by the drugs (never proven to be effective or approved by the FDA for treating neurodegeneration of the type I have) that I am prescribed off-label by well-intentioned doctors hoping that I could be one of a tiny group for whom the drugs might work, at least a little for a little while. Pretty much all of the time I am glad I conducted my studies using my accumulated skills from 35 years. I am very confident that I have accurately identified what works for me. The “problem” is that there is no guarantee that my experience will be your experience. More and larger studies may be able to determine how robust my findings are and whether they can be generalized to different types of individuals with various types of dementia. My own work does not lead directly to medical or psychological advice and you should ALWAYS consult a physician or other licensed medical provider to obtain treatment.
Click on the image to expand it.

The following slide presentation shows the mind map in smaller sections. The presentation will run automatically or you might wish to click the pause button in the presentation and manually navigate through the presentation using the right and left arrow keys.
This is my last research project of a very productive research career. I am proud of it. If you think the work is worth knowing about, I hope you will use the various forms of social media to point others toward this blog and specifically toward the dementia posts. I plan to continue the one subject study as long as I can.
One final note. Most of the methods of living well with dementia I test are relatively inexpensive (less than the cost of one cup of gourmet coffee a day in a coffee shop if you do not already own a PC or Mac or tablet computer which undoubted you do as you are reading this blog). If you own a PC or Mac or tablet, I estimate the cost to apply or use the techniques is less than the cost of one plain-ole old-fashioned coffee without the designer name or copper tubes. These costs should be within the means of most people with dementia or pensioners with at most, a small lifestyle change required.



The title does evoke a lot of imagery doesn’t it? And don’t tell me you love scary roller coasters. Based on my own experience over the last few years, I can guarantee you would not like this one. This roller coaster is guaranteed to terrify you and the terror only goes away for small stretches. And you cannot get off. Ever. Or at least until dedicated researchers find a cure or way to control the symptoms and further decline in dementia effectively.
The periods when you are not falling can be pretty good. But on a roller coaster you always know that at some time that big climb or plateau is going to be followed by a pretty long and “novel” period of terror. Sometimes you are in free fall with no gravity stabilizing you.
A mind map …
Click the image to expand it.
And, by the way, I have hated scary roller coasters my whole life. Now I face one where there is no firm ground to look forward to. Or an end for the rest of my life.
Caregivers and family and friends, a friendly environment, and especially attempts to fight back and control your terror provide the moments of stability in the ride that make it tolerable, at least for a while. You can stay on the ride. Hold on tight.

The presentation presents the mind map above piece-by-piece. It will run automatically. To run it manually, push the pause button on the presentation and use the arrow keys to move between slides.
With a little help from your friends you can tame the roller coaster enough to stay on the train. You can live well with dementia even if you are in the middle of the roller coaster ride. I have. Just keep your hands on the safety bar.
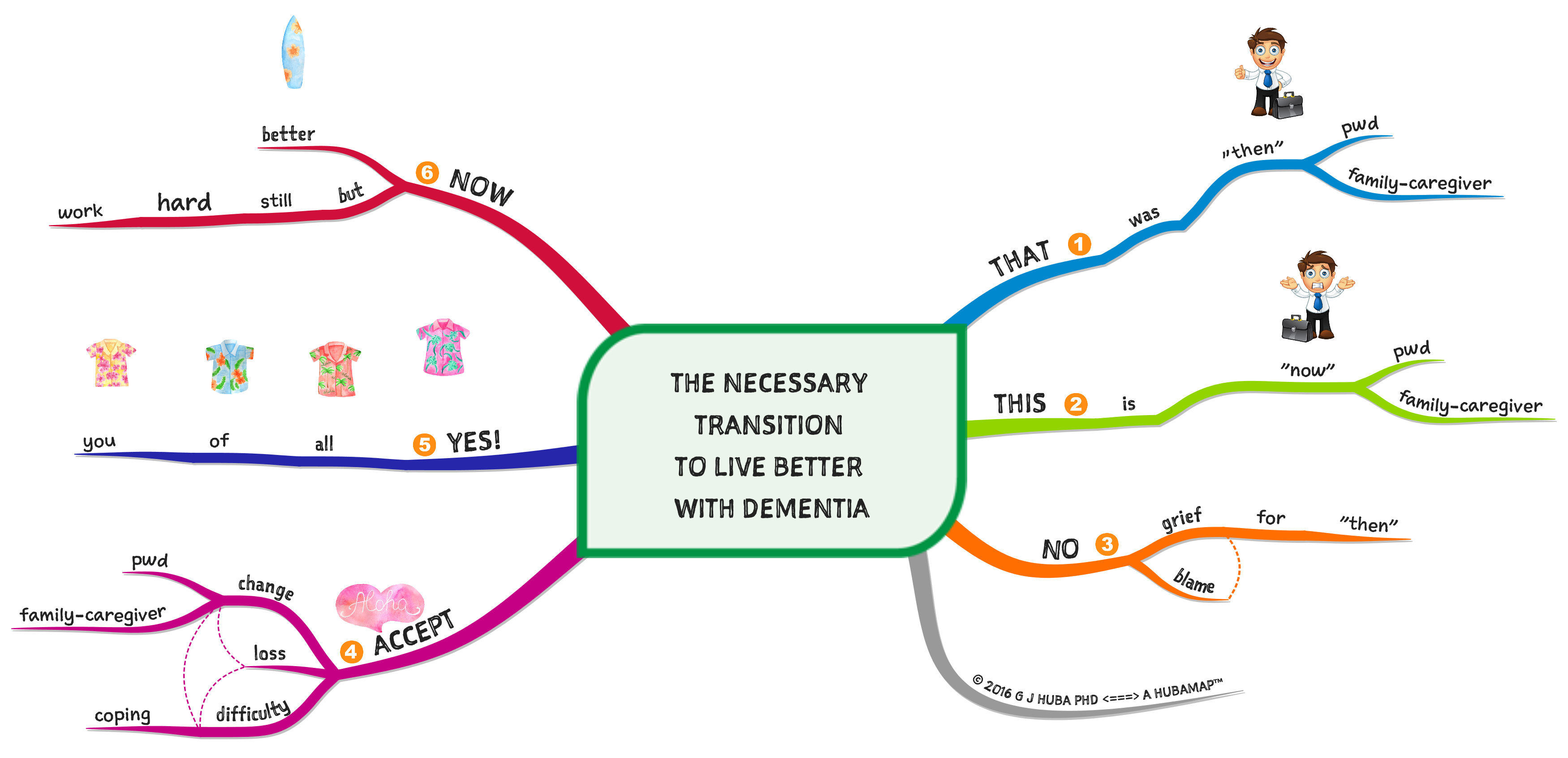
This is not psychological advice. If you are inclined to make a transition in how you think and behave, consult your doctor or a licensed mental health professional. My suggestions are ones that I believe have worked for me. They may or may not apply to you and you will not know if change is a good idea or not for you unless you consult with a qualified medical or mental health professional.
To live better and to live well, you probably need to make the transition from thinking how things were or could have been THEN and deal with the fact that this is NOW and no amount of wishful thinking is going to make things the way were before dementia hit you or someone for whom you provide care. It will never be easy for anyone to deal with dementia but you can probably make a transition if you are willing to let go of the past.
A few issues in making the change are in the mind map below. Click on it to make the map larger and to zoom in.
Note. PWD (or pwd) means person with dementia.
This presentation focuses in on parts of the map above. It will run automatically. If you would like to go through at your own pace, hit the pause button and then the arrow keys to manually move among the slides.
Click the mind map to expand its size.
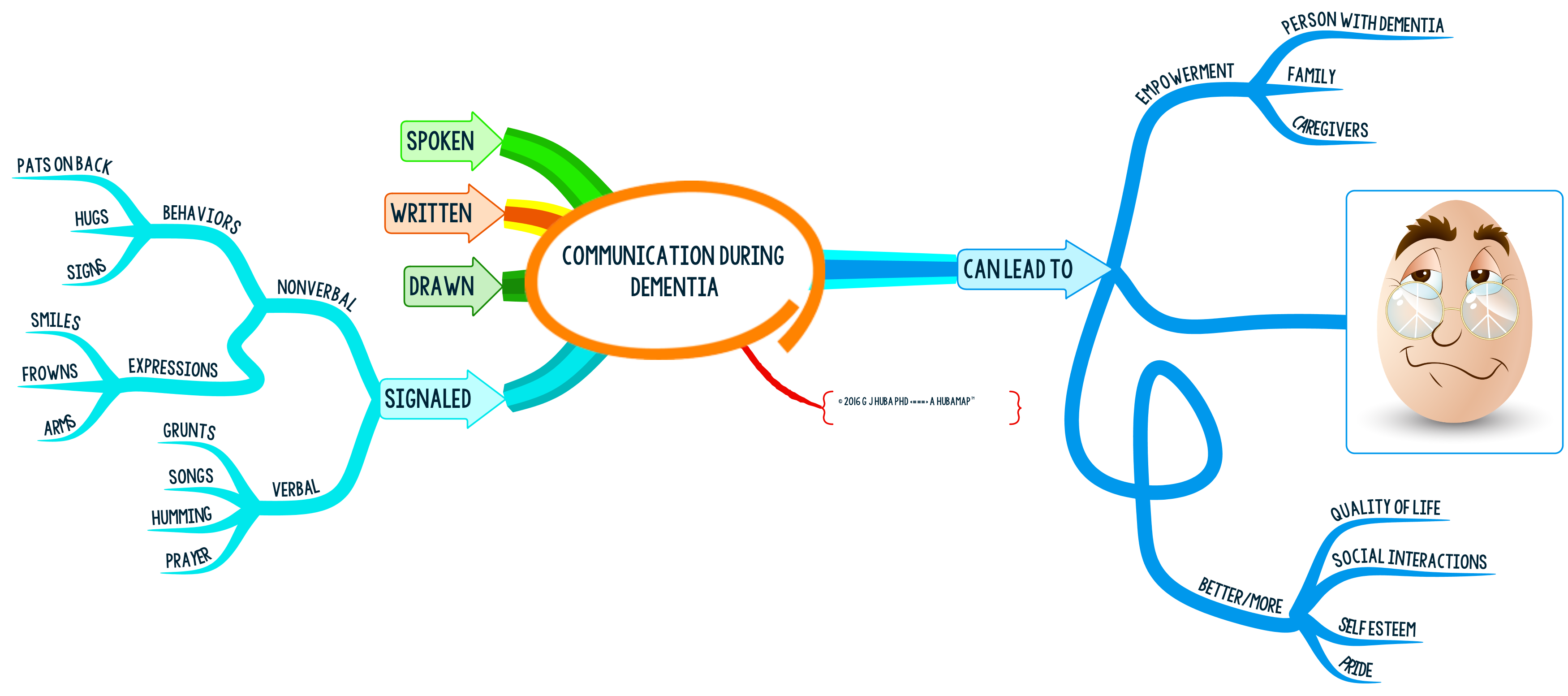
If you are a person with dementia (PWD) there are many ways you can communicate with the world besides speaking. Write. Draw. Wave your hands in wild enthusiasm. Smile. Hug.
If you are a family member or paid caregiver, speak (but even if understood) but also write, draw, and signal. It never hurts to communicate through several channels so that your message is heard.
Better communication can make the dementia experience better for both the person with dementia struggling to remember words or speak clearly or follow normal (rapid) conversation and a caregiver/family member struggling to communicate unambiguously with the person with dementia. At times, the spoken word may be the least effective of the ways to communicate.
Because of my cognitive impairment I started to use mind mapping to communicate and assist me in thinking in 2010.
Click image to expand.
The following presentation breaks the mind map above into more manageable pieces. It will run automatically or you can click the pause button and then go through the presentation manually using the arrow keys.
This what I tried to do at times over five years when I felt “destroyed” by increasing cognitive impairment.
It helped me. “Looking down?” Try to “look up.” It feels a lot better.

Try to do some great things, whether small or big. You can feel better. Just saying hello to a stranger or friend or beaming because of the sunny day or being helpful in some small way will make you and others feel better.
Don’t worry about what you lost. Rejoice that you can still help make things better.
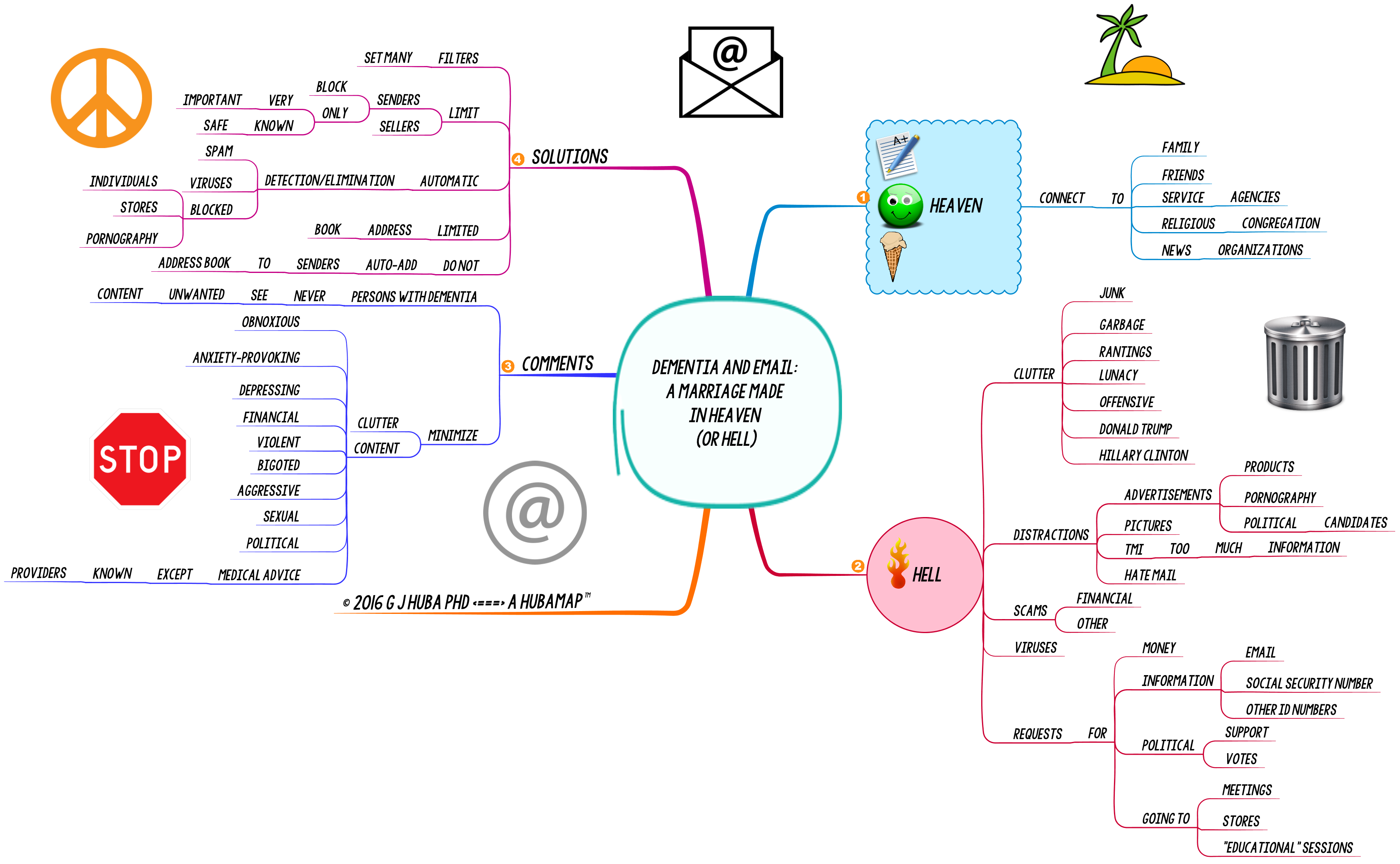
On the one end of the scale there is continued communication with family, friends, your own doctors and nurses, social agencies, and your religious congregation and various news services that send out alerts. The angels sing.
On the other hand, there is SPAM. Tons of it. Fraud. Get rich quick scams. Identify theft. Porn. Violence. Donald Trump. Hillary Clinton. Requests for cash for just about every fraudulent charity you can think of. Fake home improvement services. Fake churches. Fake food for fake children. Many of these people are flirting with unpleasant consequences.
Bad people target vulnerable people via email. People with dementia are vulnerable no matter how they look or talk or interact. They tend to trust too much, get distracted by clutter, waste time, and be more sensitive to others in need.
The situation. Some suggested solutions. Get the spam and other filters on the email and make sure they stay there. Greatly limit the amount of email that comes in.
Click on this mind map to expand it.
The slide presentation splits the mind map up into pieces that might be easier to understand. The slide advance automatically or you can hit the pause button and use the arrow keys to navigate through the presentation manually.
Living with dementia is all about improving quality of life (QOL). Treatments to fix up your brain are still in development. They will not happen in my lifetime. But, as I always suggest in this blog, there are some ways of using simple cognitive and behavioral methods that may make your life (and that of your family) more pleasant. When you have dementia, a better day is priceless.
There are several products on the Apple app store for iPhones and iPads that claim to promote electronic communications among patients, family members, and paid caregivers. In reviewing many, I found them — as a group — to be somewhat expensive and typically fairly difficult to use (by me, a member of the patient target group with a PhD and 25+ years of software development experience).
I have carried an iPhone and iPad with me almost continually for the past 10 years. I have always considered the voice control app Siri to be something of a “bar toy” that you can ask questions like “who won the 1923 World Series?” or “what is the dollar-euro exchange rate?” My judgment had been drawn based on the earliest versions of Siri that had significant problems in voice recognition and returned “interesting if bizarre” information in response to questions.
Then recently I watched a teen sit with her iPhone and take notes, schedule, get smart answers, and generally zip through her homework. She did not seem to be doing anything “special” to enable the phone to interpret her voice. And she got terrific and accurate translation of her spoken words into written words using Siri.
Well … I decided it was time to start acting “cool” and flexible again and seem like I was having a conversation with my friend Siri. I started to talk to Siri and “her/him/it” and tell it to take written notes. I experimented with several Apple devices and found that multiple individuals (and devices) linked on the same account can easily share notes.
Free. Nothing special required. Easy. Doing a little research, I concluded that the transcription and note taking function now work far better than ever before due to enhancements in Siri, but more importantly because of recent upgrades in the Notes app included in iOS.
There is huge potential here for Persons with Dementia to take notes for themselves easily and simply by speaking into an iPhone they carry everywhere. And for caregivers and family members to leave notes for a Person with Dementia. Or to check the PWD’s notes to see what is going on. No lost notes and I bet that many people are likely to carry their phone everywhere than to carry a pencil and notepad.
If you and Mom (or Dad or your aging friends) carry iPhones, you can easily set up a system where notes can be shared in a couple of minutes.
Comments:
1. Apple is reliably rumored to be releasing Siri for the Mac in June 2016.
2. At this time I only recommend sharing notes, not calendars. Calendars are confusing.
3. Siri also runs on the Apple Watch. Hopefully well enough to also share notes.
4. Donald Trump is reportedly suing to change the name Siri because he does not want Syrians in the US (OK, so I couldn’t resist).
The mind map below organizes the basic information about this system and provides additional details.

The slide presentation breaks the mind map into pieces. It will run automatically or you can push the pause button and then use the arrow keys to move through the presentation manually.
Siri, take a note. Get started making electronic notes with Siri many times per day.
You can change voices for Siri [male/female and in the US Version Americanish, UKish, or Australish] easily. I prefer the female British voice (the American female version is too common, the Australian female version is too upbeat and hard to follow, and I do not want a male butler or a bossy service representative voice). Mary Poppins is quite helpful, friendly, and at times scolds you. I need a nanny.
By the way, ask Siri to take a note and say this word. It will spell it correctly.
If you use Siri, you can also find out the answer to the “argument” (discussion) you having with your caregiver about how much money Lionel Messi makes in dollars, euros, pounds, or yen.
Sorry folks. I do not use PCs anymore after 30 years of frustration and bugs or Android devices so if you do not use Apple products you are going to need to explore this area on your own.





















