Let’s be honest, there is not enough empirical, hard scientific evidence that mind map based learning programs are as effective as there should be. In fact there is FAR less evidence to support efficacy claims about mind mapping than there should be. This has to be fixed.
Before the mind mappers start cursing me out, put this into context — I strongly support mind mapping and think it should be used far more than it is But I cannot find specific studies that strongly support efficacy.
Don’t flip the channel yet … I am now going to give you the most valuable free consulting I have ever provided anyone.
A few studies give people some training into “who knows what” mind mapping and see if they remember or “learn who knows what” better. Creativity is not measured, communication is not measured, long-term efficacy is not measured, training clinical practice efficacy is not measured, and many other aspects of cognitive enhancement claimed are not measured. Still, I believe that mind mapping is useful for most of these things and mind mapping works.
Now “prove” it.
Here is the biggest reason why mind mapping has not been shown to work in anything approaching a “definitive” scientific study or unbiased evaluation — too many things are called “mind mapping” are all lumped together.
A strong research (evaluation) design includes the following factors.
a) Different things called mind mapping are compared. As I see it, there is are three major things called “mind mapping.” The first is Buzan-style organic mind mapping. My bias is to say that this will work best in most (but not all) applications, but I would like to see hard data that my observations are correct. The second style of mind mapping is that embraced by those who use Mindjet aka Mind Manager and comparable programs. Such a style seems to be preferred among business types, and I used Mindjet (formerly known as Mind Manager) for about 15-20 years with many different types of health- and social-care professionals. Then there are dozens of other methods and diagrams called “mind maps,” most of which probably could be called spider maps. I would clump all of these methods together although I do recognize that the category is very heterogeneous.
Addition to original post: Separating these three categories will almost certainly show that the three clusters of methods are not equally effective for all applications. Combining them together dilutes the effects of the first and second methods because the third is probably comprised of a number of less than effective methods.
b) The effects of mind mapping need to be maximized. That is, the participants learning mind mapping or being taught to read existing mind maps need to be trained by experts (and I mean real top-of-the-food-chain mind mapping instructors) in one of the three types of “mind mapping.” The instructor needs to be a “real pro” at this, not a teacher or consultant who has had minimal formal training in mind mapping. Random assignment of participants (subjects) to one of the three mind mapping conditions needs to be made.
c) A lot of before and after variables need to be measured like memory, creativity, ability to learn new materials, ability to increase upon prior knowledge, sophistication of information processing, and all of the other things people claim about mind mapping.
d) Then the data need to be analyzed for enhancements (or not) from mind mapping according in each of the three three dominant models. That is, there needs to be a study of the interactions of learning one of the three mind mapping models from an expert, type of application, and type of effects.
Show me a dozen studies that support mind mapping (with random assignment, large samples, and conducted by a neutral investigator in this highly competitive commercial area) and I will tell everyone it has been proven that mind mapping works for these 10 applications and not these 5 others and what the best kind of mind mind mapping is for achieving certain goals.
Show me even better and more complex studies and I will jump with glee that my own observations have been confirmed.
Or, if it doesn’t work, accept the fact that this is voodoo, a management-education-training fad, or just plain commercial exploitation. (I don’t believe it is any of these things but I also cannot say YET that science unequivocally understands mind mapping.)
You wanna make the big claims, get independent parties to test them in an unbiased way that meets the most rigid scientific-educational standards. The odds are you will be happy you did as will potential users and educator-trainers.
[If you are an education, psychology, neuroscience, or healthcare student there are a lot of good PhD dissertations to be written in this area.]
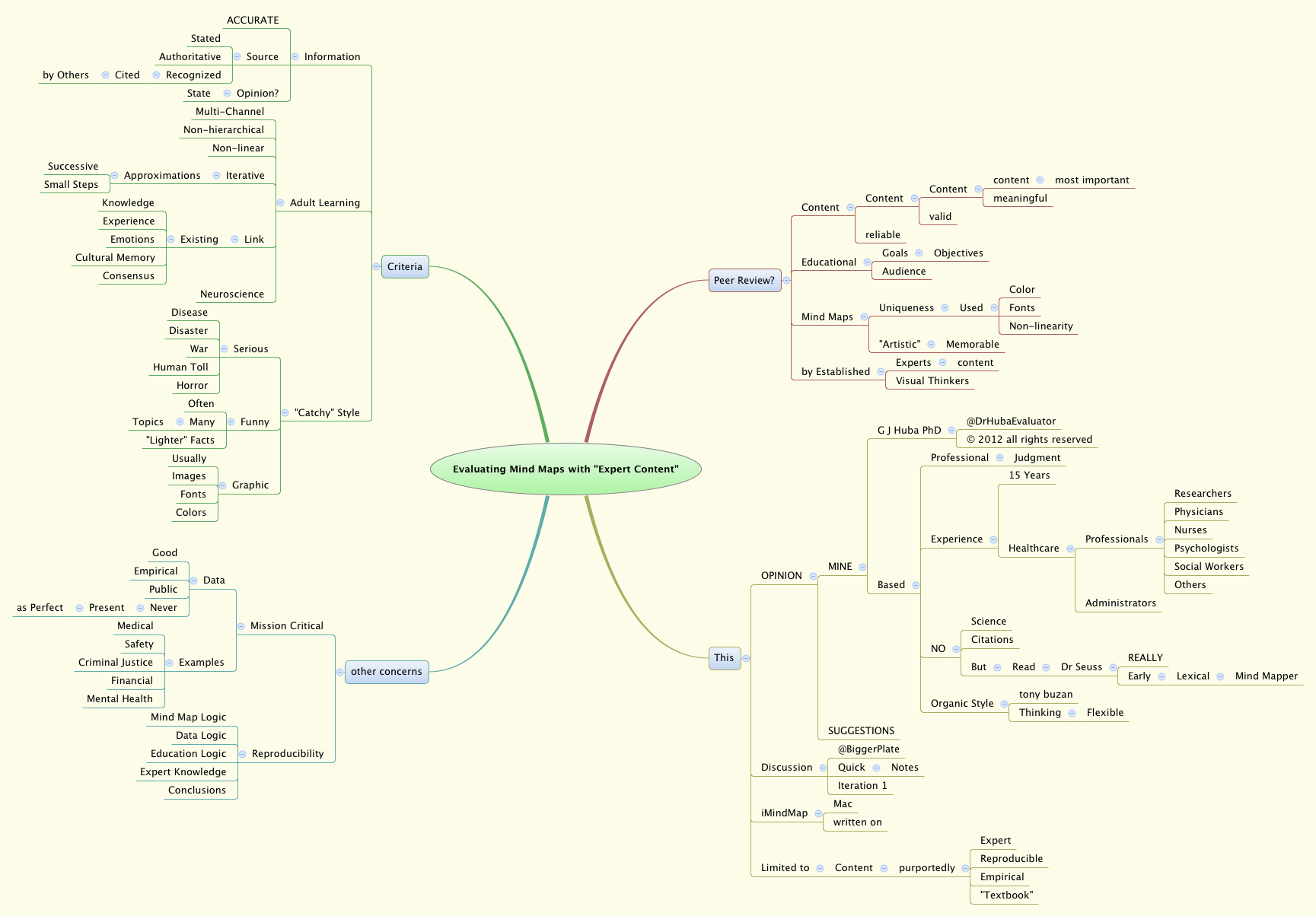
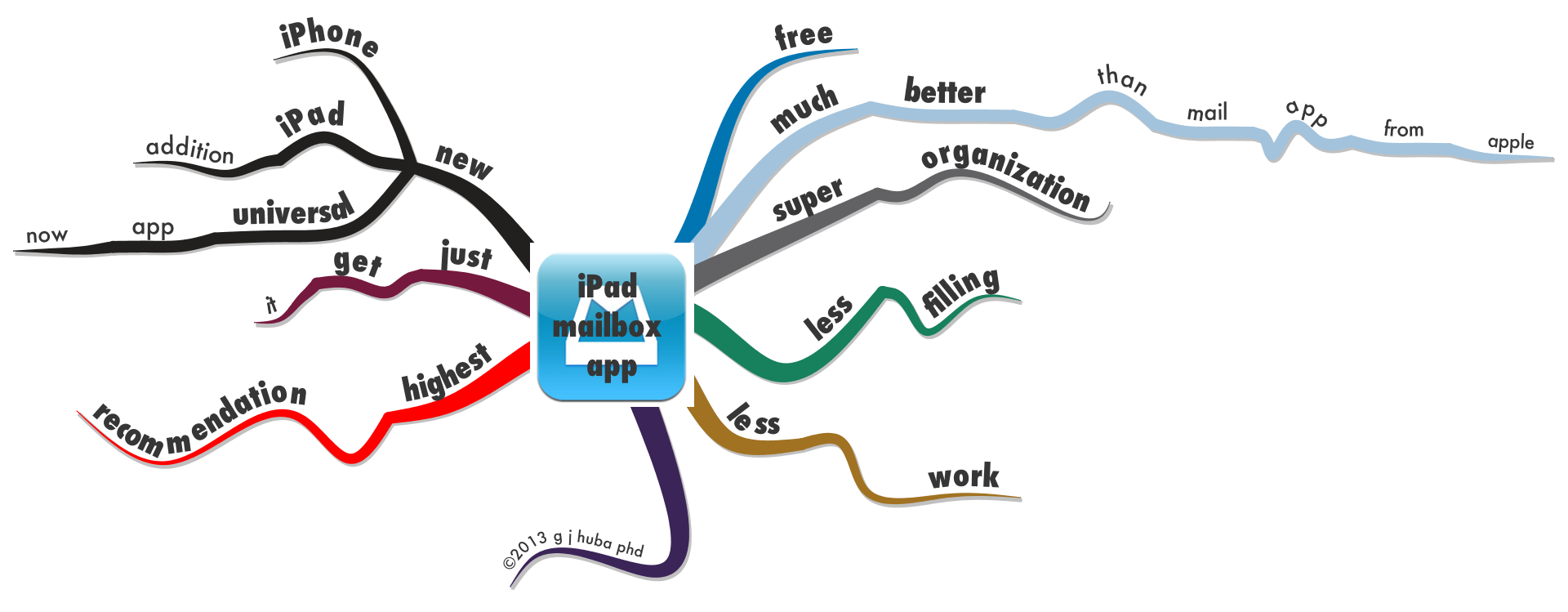
A few of my examples of using mind maps from around this blog/website.
Click images to zoom.

 comfort work 35
comfort work 35 










Like this:
Like Loading...